The George Institute for Global Health, UNSW Sydney, Sydney, New South Wales, Australia.
The George Institute for Global Health, UNSW Sydney, New Delhi, India.
PLoS Med. 2021 Mar 4;18(3):e1003485. doi: 10.1371/journal.pmed.1003485. eCollection 2021 Mar.
Global cardiovascular disease (CVD) burden is high and rising, especially in low-income and middle-income countries (LMICs). Focussing on 45 LMICs, we aimed to determine (1) the adult population's median 10-year predicted CVD risk, including its variation within countries by socio-demographic characteristics, and (2) the prevalence of self-reported blood pressure (BP) medication use among those with and without an indication for such medication as per World Health Organization (WHO) guidelines.
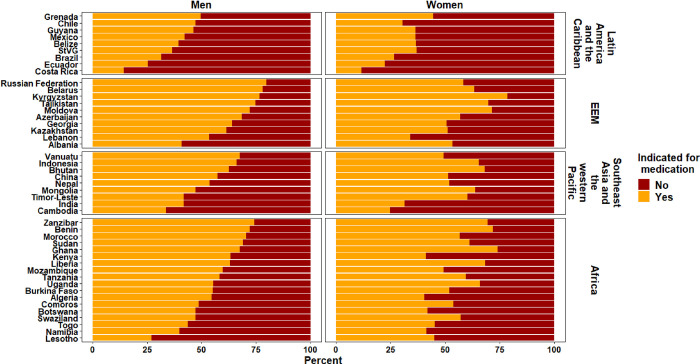
We conducted a cross-sectional analysis of nationally representative household surveys from 45 LMICs carried out between 2005 and 2017, with 32 surveys being WHO Stepwise Approach to Surveillance (STEPS) surveys. Country-specific median 10-year CVD risk was calculated using the 2019 WHO CVD Risk Chart Working Group non-laboratory-based equations. BP medication indications were based on the WHO Package of Essential Noncommunicable Disease Interventions guidelines. Regression models examined associations between CVD risk, BP medication use, and socio-demographic characteristics. Our complete case analysis included 600,484 adults from 45 countries. Median 10-year CVD risk (interquartile range [IQR]) for males and females was 2.7% (2.3%-4.2%) and 1.6% (1.3%-2.1%), respectively, with estimates indicating the lowest risk in sub-Saharan Africa and highest in Europe and the Eastern Mediterranean. Higher educational attainment and current employment were associated with lower CVD risk in most countries. Of those indicated for BP medication, the median (IQR) percentage taking medication was 24.2% (15.4%-37.2%) for males and 41.6% (23.9%-53.8%) for females. Conversely, a median (IQR) 47.1% (36.1%-58.6%) of all people taking a BP medication were not indicated for such based on CVD risk status. There was no association between BP medication use and socio-demographic characteristics in most of the 45 study countries. Study limitations include variation in country survey methods, most notably the sample age range and year of data collection, insufficient data to use the laboratory-based CVD risk equations, and an inability to determine past history of a CVD diagnosis.
This study found underuse of guideline-indicated BP medication in people with elevated CVD risk and overuse by people with lower CVD risk. Country-specific targeted policies are needed to help improve the identification and management of those at highest CVD risk.
全球心血管疾病(CVD)负担沉重且呈上升趋势,尤其是在低收入和中等收入国家(LMICs)。我们关注 45 个 LMICs,旨在确定(1)成年人的 10 年中位 CVD 风险预测值,包括各国按社会人口特征的差异,以及(2)根据世界卫生组织(WHO)指南,报告有或无血压(BP)药物治疗指征的人群中 BP 药物的使用情况。
我们对 2005 年至 2017 年间进行的 45 个 LMIC 国家的全国代表性家庭调查进行了横断面分析,其中 32 个调查是世界卫生组织逐步监测方法(STEPS)调查。使用 2019 年世界卫生组织 CVD 风险图工作组非实验室方程计算各国的特定人群 10 年 CVD 风险中位数。BP 药物的治疗指征基于世界卫生组织基本非传染性疾病综合干预包指南。回归模型研究了 CVD 风险、BP 药物使用和社会人口特征之间的关系。我们的完整病例分析包括来自 45 个国家的 600484 名成年人。男性和女性的 10 年 CVD 风险中位数(四分位距 [IQR])分别为 2.7%(2.3%-4.2%)和 1.6%(1.3%-2.1%),估计表明风险最低的是撒哈拉以南非洲,风险最高的是欧洲和东地中海。在大多数国家,较高的教育程度和当前的就业状况与较低的 CVD 风险相关。在需要接受 BP 药物治疗的人群中,男性服用药物的中位数(IQR)百分比为 24.2%(15.4%-37.2%),女性为 41.6%(23.9%-53.8%)。相反,根据 CVD 风险状况,所有服用 BP 药物的人中,中位数(IQR)有 47.1%(36.1%-58.6%)的人没有服用指征。在大多数 45 个研究国家中,BP 药物的使用与社会人口特征之间没有关联。研究的局限性包括各国调查方法的差异,尤其是样本年龄范围和数据收集年份、使用实验室 CVD 风险方程的数据不足,以及无法确定过去 CVD 诊断的病史。
本研究发现,高危 CVD 人群中指南推荐的 BP 药物使用率不足,低危 CVD 人群中使用率过高。需要针对各国的具体情况制定有针对性的政策,以帮助提高高危 CVD 人群的识别和管理水平。