Department of Global Health and Population, Harvard T.H. Chan School of Public Health, Harvard University, Boston, Massachusetts, United States of America.
Department of Medicine, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Massachusetts, United States of America.
PLoS Med. 2018 Jun 19;15(6):e1002581. doi: 10.1371/journal.pmed.1002581. eCollection 2018 Jun.
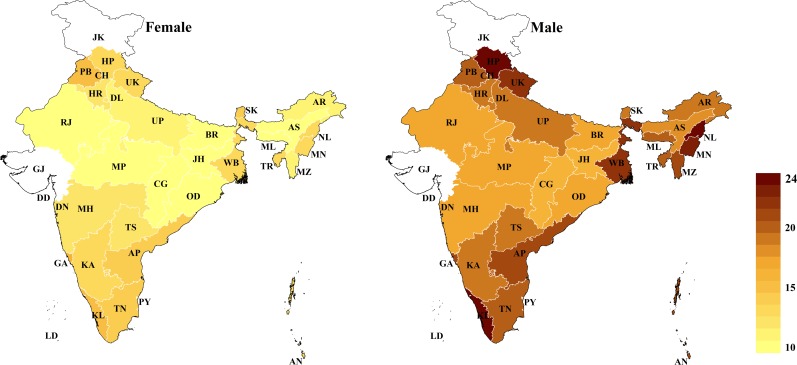
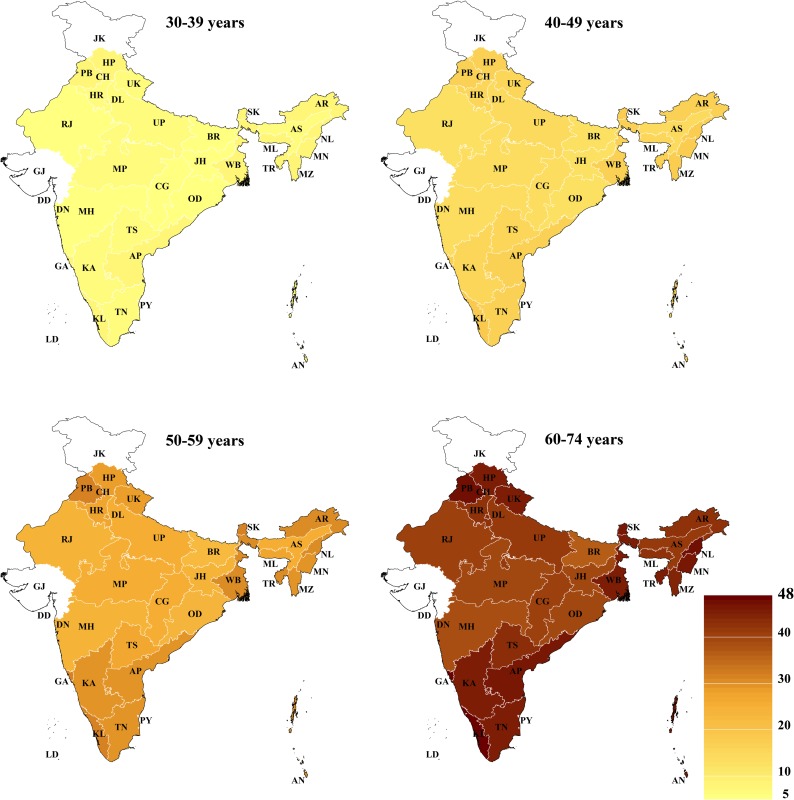
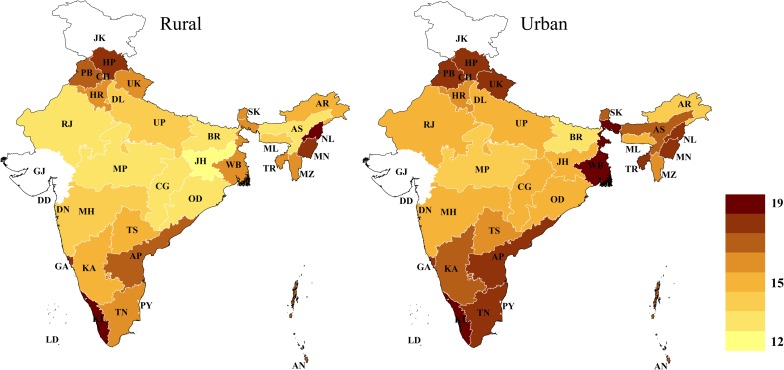
Cardiovascular disease (CVD) is the leading cause of mortality in India. Yet, evidence on the CVD risk of India's population is limited. To inform health system planning and effective targeting of interventions, this study aimed to determine how CVD risk-and the factors that determine risk-varies among states in India, by rural-urban location, and by individual-level sociodemographic characteristics.
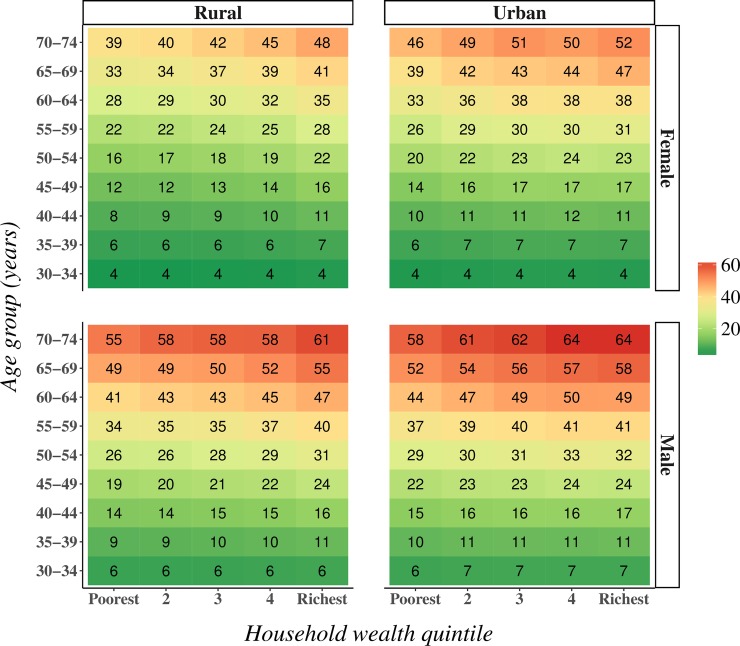
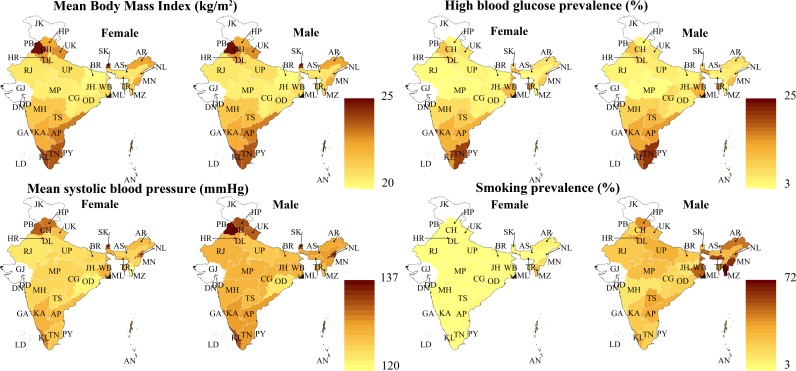
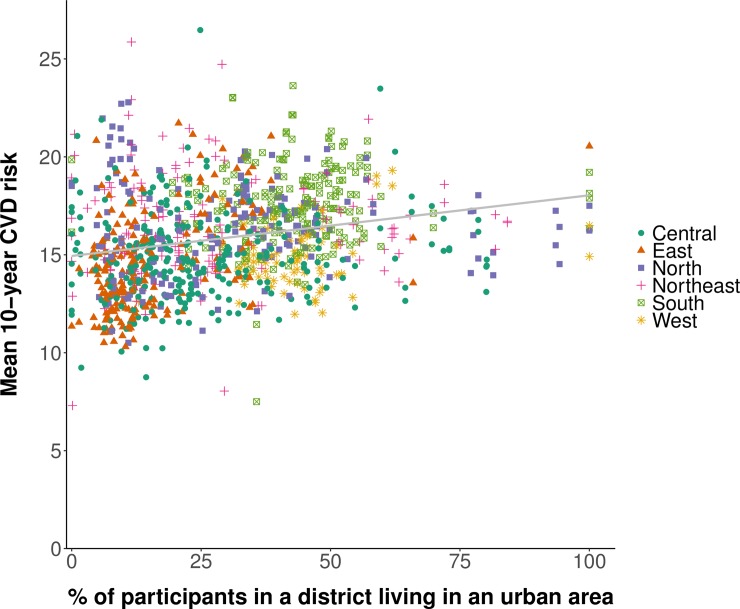
We used 2 large household surveys carried out between 2012 and 2014, which included a sample of 797,540 adults aged 30 to 74 years across India. The main outcome variable was the predicted 10-year risk of a CVD event as calculated with the Framingham risk score. The Harvard-NHANES, Globorisk, and WHO-ISH scores were used in secondary analyses. CVD risk and the prevalence of CVD risk factors were examined by state, rural-urban residence, age, sex, household wealth, and education. Mean CVD risk varied from 13.2% (95% CI: 12.7%-13.6%) in Jharkhand to 19.5% (95% CI: 19.1%-19.9%) in Kerala. CVD risk tended to be highest in North, Northeast, and South India. District-level wealth quintile (based on median household wealth in a district) and urbanization were both positively associated with CVD risk. Similarly, household wealth quintile and living in an urban area were positively associated with CVD risk among both sexes, but the associations were stronger among women than men. Smoking was more prevalent in poorer household wealth quintiles and in rural areas, whereas body mass index, high blood glucose, and systolic blood pressure were positively associated with household wealth and urban location. Men had a substantially higher (age-standardized) smoking prevalence (26.2% [95% CI: 25.7%-26.7%] versus 1.8% [95% CI: 1.7%-1.9%]) and mean systolic blood pressure (126.9 mm Hg [95% CI: 126.7-127.1] versus 124.3 mm Hg [95% CI: 124.1-124.5]) than women. Important limitations of this analysis are the high proportion of missing values (27.1%) in the main outcome variable, assessment of diabetes through a 1-time capillary blood glucose measurement, and the inability to exclude participants with a current or previous CVD event.
This study identified substantial variation in CVD risk among states and sociodemographic groups in India-findings that can facilitate effective targeting of CVD programs to those most at risk and most in need. While the CVD risk scores used have not been validated in South Asian populations, the patterns of variation in CVD risk among the Indian population were similar across all 4 risk scoring systems.
心血管疾病(CVD)是印度的主要死亡原因。然而,关于印度人口 CVD 风险的证据有限。为了为卫生系统规划和有效干预措施提供信息,本研究旨在确定 CVD 风险在印度各邦之间的差异,以及农村-城市地区和个体社会人口特征的差异,以及确定风险的因素。
我们使用了 2012 年至 2014 年间进行的 2 项大型家庭调查,其中包括印度各地 797540 名 30 至 74 岁成年人的样本。主要结局变量是根据弗雷明汉风险评分计算的 10 年内 CVD 事件的预测风险。哈佛- NHANES、Globorisk 和世卫组织-ISH 评分用于二次分析。通过邦、城乡居住、年龄、性别、家庭财富和教育水平来检查 CVD 风险和 CVD 风险因素的患病率。CVD 风险从恰蒂斯加尔邦的 13.2%(95%CI:12.7%-13.6%)到喀拉拉邦的 19.5%(95%CI:19.1%-19.9%)不等。印度北部、东北部和南部的 CVD 风险往往最高。地区级财富五分位数(根据地区内中位数家庭财富确定)和城市化水平均与 CVD 风险呈正相关。同样,在男女两性中,家庭财富五分位数和居住在城市地区均与 CVD 风险呈正相关,但在女性中的相关性强于男性。在较贫穷的家庭财富五分位数和农村地区,吸烟更为普遍,而体重指数、高血糖和收缩压与家庭财富和城市位置呈正相关。男性的吸烟率(标准化后)明显更高(26.2%[95%CI:25.7%-26.7%]与 1.8%[95%CI:1.7%-1.9%])和平均收缩压(126.9mmHg[95%CI:126.7-127.1]与 124.3mmHg[95%CI:124.1-124.5])高于女性。本分析的重要局限性是主要结局变量中存在较高比例的缺失值(27.1%)、通过 1 次毛细血管血糖测量评估糖尿病以及无法排除当前或既往 CVD 事件的参与者。
本研究发现,印度各邦和社会人口群体之间的 CVD 风险存在很大差异,这可以为最有风险和最需要的 CVD 计划提供有效目标。虽然南亚人群中尚未验证 CVD 风险评分,但印度人群中 CVD 风险的变化模式在所有 4 种风险评分系统中相似。