Dönmez Tugba, Höhne Kerstin, Zissel Gernot, Herrmann Ken, Hautzel Hubertus, Aigner Clemens, Hegedüs Balazs, Ploenes Till
Department of Thoracic Surgery and Endoscopy, Ruhrlandklinik, West German Cancer Center, University Hospital, University of Duisburg-Essen, Essen, Germany.
Department of Pneumology, Medical Center - University of Freiburg, Freiburg, Faculty of Medicine, University of Freiburg, Freiburg Germany.
Data Brief. 2021 Feb 18;35:106859. doi: 10.1016/j.dib.2021.106859. eCollection 2021 Apr.
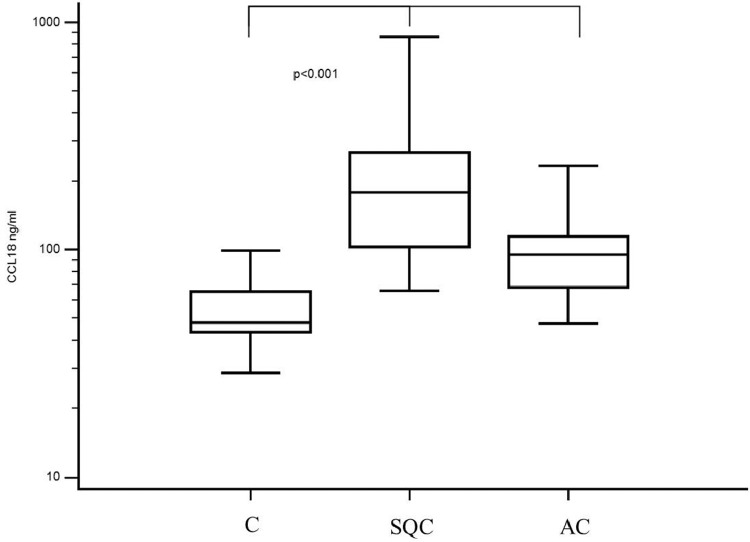
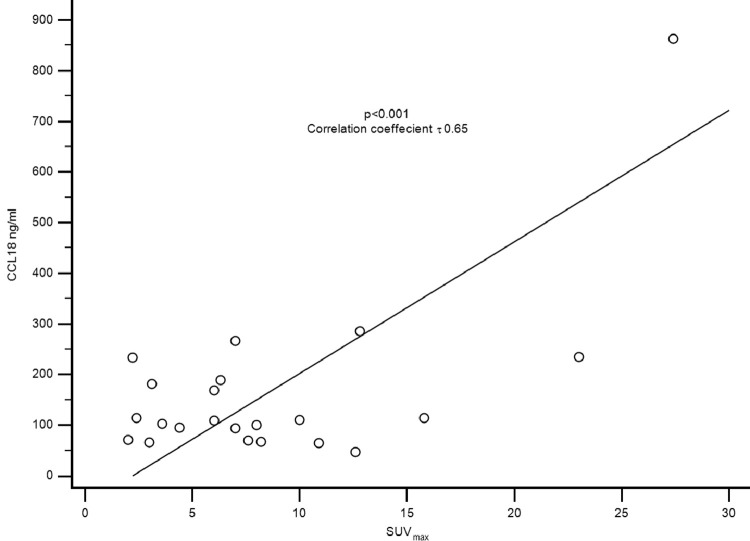
Non-small cell lung cancer (NSCLC) is one of the most common malignancies in the western world [1]. Despite multiple therapeutic and diagnostic advances, the overall survival is low and recurrence of NSCLC is a common problem with different treatment regimens. The inclusion of fluorine fluorodeoxyglucose (FDG) positron emission tomography (PET) in combination with computed tomography (CT) in clinical practice was revolutionary for the staging of NSCLC [2]. FDG-PET/CT provides morphological, functional, and metabolic information about the tumor, which is usually highly, metabolically active. Due to the increased glucose uptake, FDG is actively accumulatedin the tumor tissues, resulting in an increased standardized uptake value (SUV). The tumor tissue itself consists of neoplastic cells, extracellular matrix, fibroblasts, and various immune cells. These immune cells include tumor-infiltrating lymphocytes, regulatory T cells, and macrophages. Macrophages have different activation patterns and play an essential role in inflammation and cancer. In particular, tumor-associated macrophages (TAMs) are a specialized group of alternatively activated or M2 macrophages. TAMs release several chemokines that are different from those released by classically activated macrophages found in an inflammatory environment. One of the most important chemokines released by TAMs is CC-chemokine ligand 18 (CCL18). Although CCL18 is present in healthy subjects, its levels are significantly elevated in the serum of patients with NSCLC. It correlates with overall survival and tumor stage in several malignant diseases [3,4]. A recurring problem is that increased glucose metabolism can be found in the inflammatory tissue, which can also lead to an increased SUV in FDG PET/CT, lowering its oncological specificity [5]. In a previous study, we demonstrated that serum CCL18 levels can be used to differentiate between patients with NSCLC and healthy subjects [3]. Hence, we investigated the correlation between serum CCL18 levels and the maximum standardized uptake value (SUV) of the primary tumor using FDG-PET/CT. We found a significant correlation between the SUV of the primary tumor and the serum CCL18 level. The data are important because they can be used to draw conclusions about immunometabolism. Furthermore, they can serve as basis for future prospective clinical studies.
非小细胞肺癌(NSCLC)是西方世界最常见的恶性肿瘤之一[1]。尽管在治疗和诊断方面取得了多项进展,但NSCLC的总体生存率较低,且不同治疗方案下NSCLC复发是一个常见问题。在临床实践中,将氟脱氧葡萄糖(FDG)正电子发射断层扫描(PET)与计算机断层扫描(CT)相结合,对NSCLC的分期具有革命性意义[2]。FDG-PET/CT可提供有关肿瘤的形态、功能和代谢信息,肿瘤通常具有较高的代谢活性。由于葡萄糖摄取增加,FDG在肿瘤组织中被主动积聚,导致标准化摄取值(SUV)升高。肿瘤组织本身由肿瘤细胞、细胞外基质、成纤维细胞和各种免疫细胞组成。这些免疫细胞包括肿瘤浸润淋巴细胞、调节性T细胞和巨噬细胞。巨噬细胞具有不同的激活模式,在炎症和癌症中起重要作用。特别是,肿瘤相关巨噬细胞(TAM)是一组特殊的替代性激活或M2巨噬细胞。TAM释放几种不同于炎症环境中经典激活巨噬细胞释放的趋化因子。TAM释放的最重要趋化因子之一是CC趋化因子配体18(CCL18)。虽然CCL18在健康受试者中也存在,但其水平在NSCLC患者血清中显著升高。它与几种恶性疾病的总体生存率和肿瘤分期相关[3,4]。一个反复出现的问题是,炎症组织中也可发现葡萄糖代谢增加,这也可导致FDG PET/CT中的SUV升高,从而降低其肿瘤学特异性[5]。在先前的一项研究中,我们证明血清CCL18水平可用于区分NSCLC患者和健康受试者[3]。因此,我们使用FDG-PET/CT研究了血清CCL18水平与原发性肿瘤最大标准化摄取值(SUV)之间的相关性。我们发现原发性肿瘤的SUV与血清CCL18水平之间存在显著相关性。这些数据很重要,因为它们可用于得出关于免疫代谢的结论。此外,它们可作为未来前瞻性临床研究的基础。