Schurtz Guillaume, Rousse Natacha, Saura Ouriel, Balmette Vincent, Vincent Flavien, Lamblin Nicolas, Porouchani Sina, Verdier Basile, Puymirat Etienne, Robin Emmanuel, Van Belle Eric, Vincentelli André, Aissaoui Nadia, Delhaye Cédric, Delmas Clément, Cosenza Alessandro, Bonello Laurent, Juthier Francis, Moussa Mouhamed Djahoum, Lemesle Gilles
Cardiac Intensive Care Unit, Heart and Lung Institute, CHU Lille, 59000 Lille, France.
Department of Interventional Cardiology for Coronary, Valves and Structural Heart Diseases, CHU Lille, Institut Coeur Poumon, Cardiology, 59000 Lille, France.
J Clin Med. 2021 Feb 14;10(4):759. doi: 10.3390/jcm10040759.
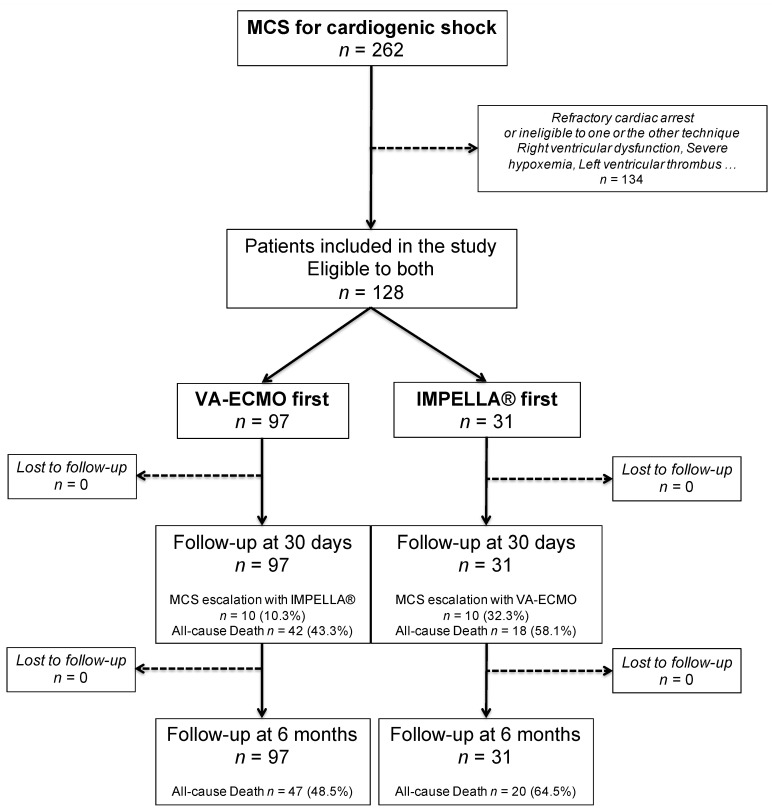
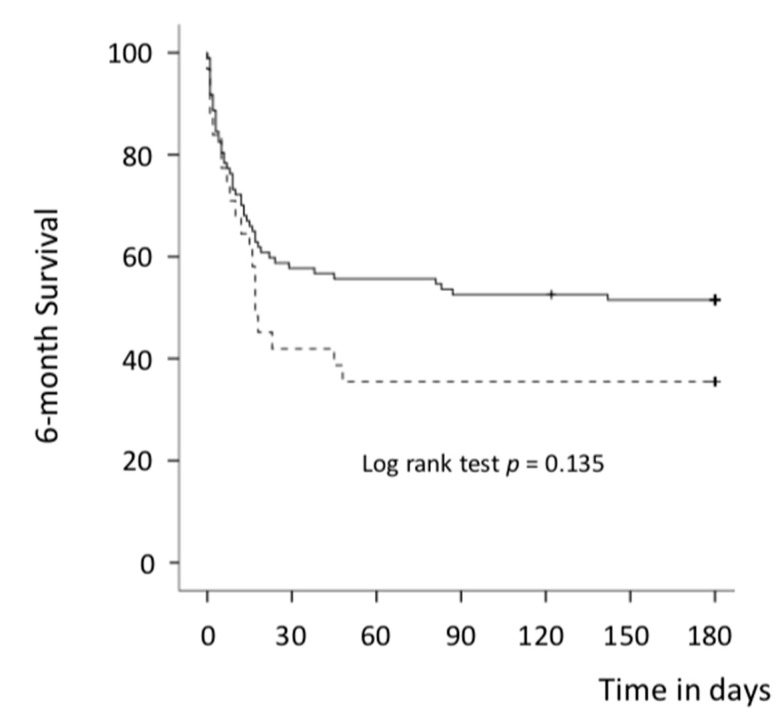
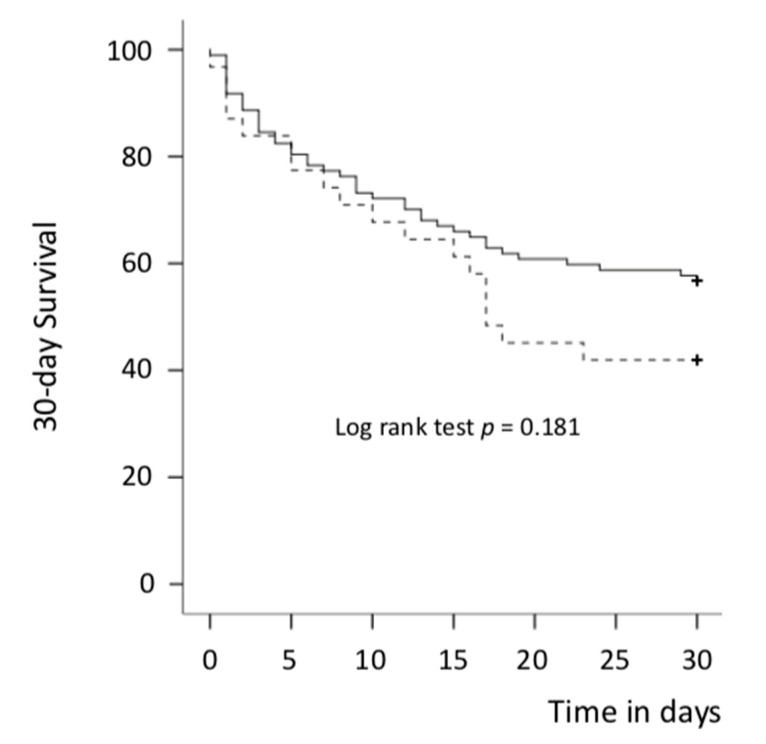
Mechanical circulatory support (MCS) devices are effective tools in managing refractory cardiogenic shock (CS). Data comparing veno-arterial extracorporeal membrane oxygenation (VA-ECMO) and IMPELLA are however scarce. We aimed to assess outcomes of patients implanted with these two devices and eligible to both systems. From 2004 to 2020, we retrospectively analyzed 128 patients who underwent VA-ECMO or IMPELLA in our institution for refractory left ventricle (LV) dominant CS. All patients were eligible to both systems: 97 patients were first implanted with VA-ECMO and 31 with IMPELLA. The primary endpoint was 30-day all-cause death. VA-ECMO patients were younger (52 vs. 59.4, = 0.006) and had a higher lactate level at baseline than those in the IMPELLA group (6.84 vs. 3.03 mmol/L, < 0.001). Duration of MCS was similar between groups (9.4 days vs. 6 days in the VA-ECMO and IMPELLA groups respectively, = 0.077). In unadjusted analysis, no significant difference was observed between groups in 30-day mortality: 43.3% vs. 58.1% in the VA-ECMO and IMPELLA groups, respectively ( = 0.152). After adjustment, VA-ECMO was associated with a significant reduction in 30-day mortality (HR = 0.25, = 0.004). A higher rate of MCS escalation was observed in the IMPELLA group: 32.3% vs. 10.3% ( = 0.003). In patients eligible to either VA-ECMO or IMPELLA for LV dominant refractory CS, VA-ECMO was associated with improved survival rate and a lower need for escalation.
机械循环支持(MCS)设备是治疗难治性心源性休克(CS)的有效工具。然而,比较静脉-动脉体外膜肺氧合(VA-ECMO)和Impella的相关数据却很匮乏。我们旨在评估植入这两种设备且适用于这两种系统的患者的治疗结果。2004年至2020年期间,我们对在本机构接受VA-ECMO或Impella治疗难治性左心室(LV)为主的CS的128例患者进行了回顾性分析。所有患者均适用于这两种系统:97例患者首先植入VA-ECMO,31例植入Impella。主要终点是30天全因死亡。VA-ECMO组患者较年轻(52岁对59.4岁,P = 0.006),且基线时乳酸水平高于Impella组(6.84 mmol/L对3.03 mmol/L,P < 0.001)。两组的MCS持续时间相似(VA-ECMO组和Impella组分别为9.4天和6天,P = 0.077)。在未调整分析中,两组30天死亡率无显著差异:VA-ECMO组和Impella组分别为43.3%和58.1%(P = 0.152)。调整后,VA-ECMO与30天死亡率显著降低相关(HR = 0.25,P = 0.004)。Impella组观察到更高的MCS升级率:32.3%对10.3%(P = 0.003)。在适用于VA-ECMO或Impella治疗LV为主的难治性CS的患者中,VA-ECMO与生存率提高和升级需求降低相关。