Foerster Robert, Zwahlen Daniel Rudolf, Buchali Andre, Tang Hongjian, Schroeder Christina, Windisch Paul, Vu Erwin, Akbaba Sati, Bostel Tilman, Sprave Tanja, Zamboglou Constantinos, Zilli Thomas, Stelmes Jean-Jacques, Telkhade Tejshri, Murthy Vedang
Institute for Radiation Oncology, Cantonal Hospital Winterthur (KSW), 8401 Winterthur, Switzerland.
Medical Faculty, University of Zurich (UZH), 8091 Zurich, Switzerland.
Cancers (Basel). 2021 Feb 12;13(4):759. doi: 10.3390/cancers13040759.
Radiotherapy (RT) is an established, potentially curative treatment option for all risk constellations of localized prostate cancer (PCA). Androgen deprivation therapy (ADT) and dose-escalated RT can further improve outcome in high-risk (HR) PCA. In recent years, shorter RT schedules based on hypofractionated RT have shown equal outcome. Stereotactic body radiotherapy (SBRT) is a highly conformal RT technique enabling ultra-hypofractionation which has been shown to be safe and efficient in patients with low- and intermediate-risk PCA. There is a paucity of data on the role of SBRT in HR PCA. In particular, the need for pelvic elective nodal irradiation (ENI) needs to be addressed. Therefore, we conducted a systematic review to analyze the available data on observed toxicities, ADT prescription practice, and oncological outcome to shed more light on the value of SBRT in HR PCA.
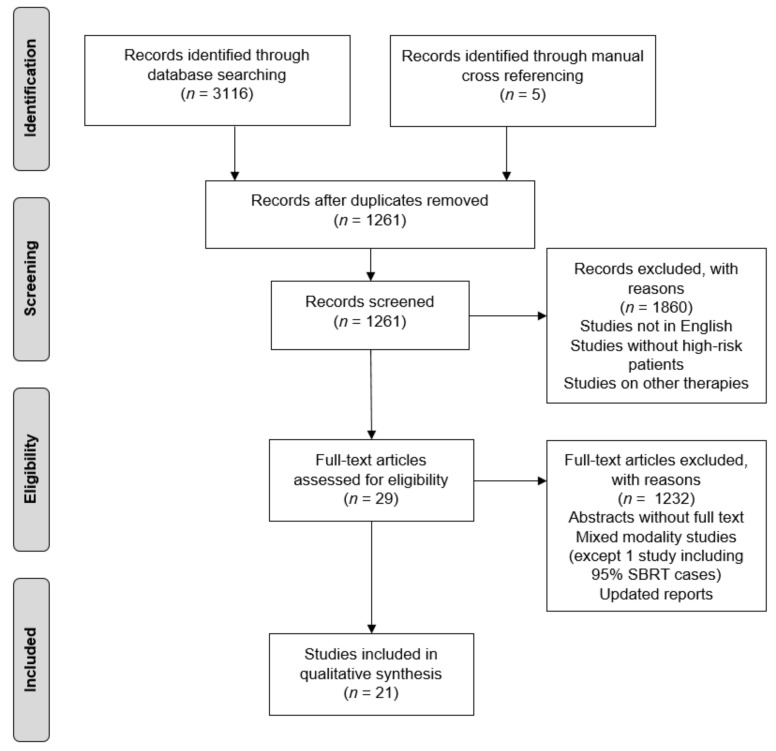
We searched the PubMed and Embase electronic databases for the terms "prostate cancer" AND "stereotactic" AND "radiotherapy" in June 2020. We adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations.
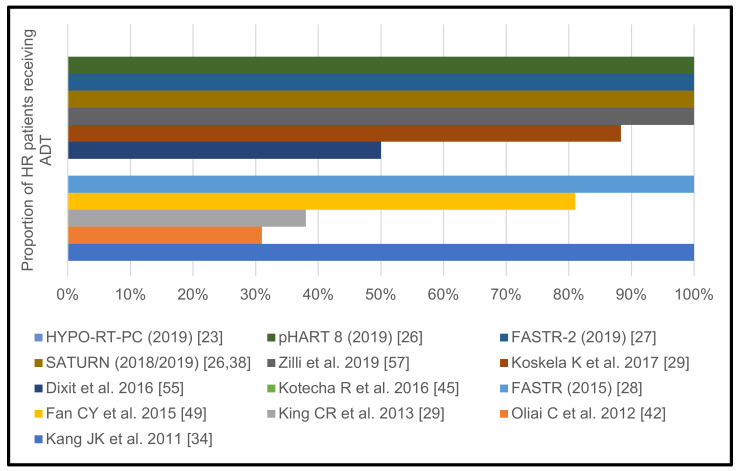
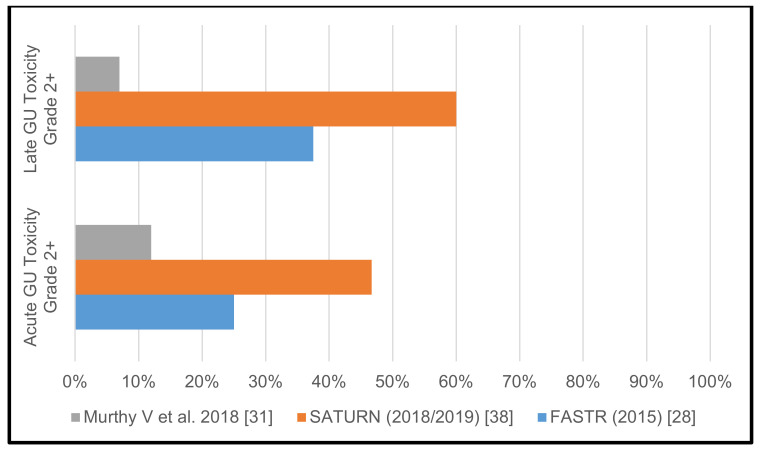
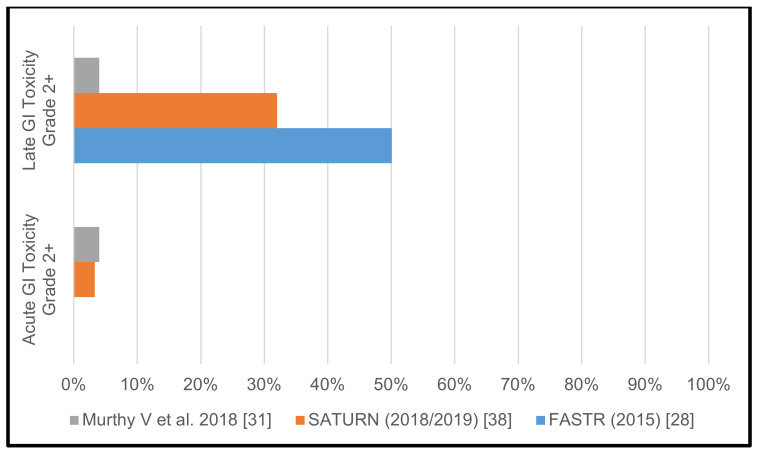
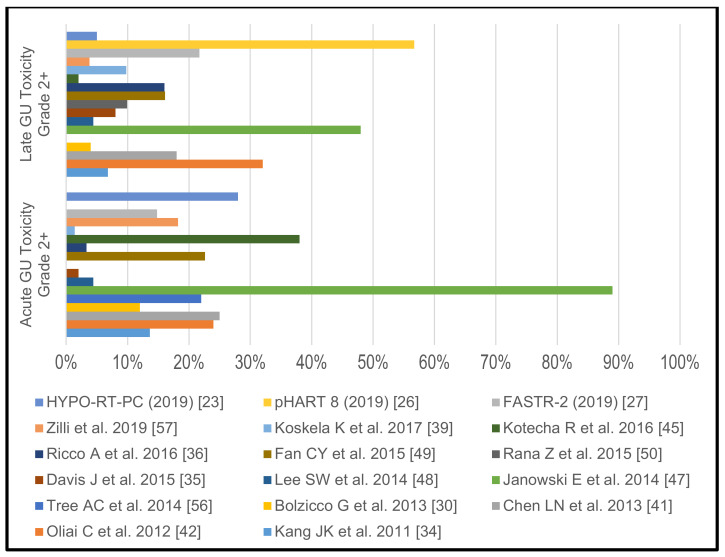
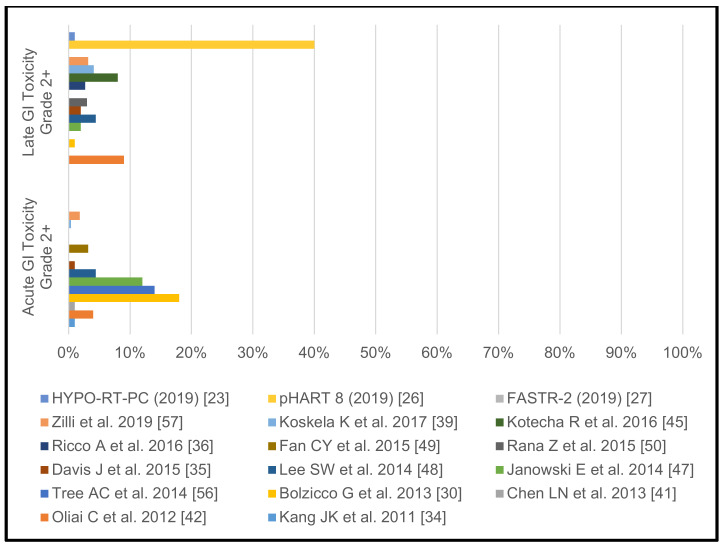
After a rigorous selection process, we identified 18 individual studies meeting all selection criteria for further analyses. Five additional studies were included because their content was judged as relevant. Three trials have reported on prostate SBRT including pelvic nodes; 2 with ENI and 1 with positive pelvic nodes only. The remaining studies investigated SBRT of the prostate only. Grade 2+ acute genitourinary (GU) toxicity was between 12% and 46.7% in the studies investigating pelvic nodes irradiation and ranged from 0% to 89% in the prostate only studies. Grade 2+ chronic GU toxicity was between 7% and 60% vs. 2% and 56.7%. Acute gastrointestinal (GI) grade 2+ toxicity was between 0% to 4% and 0% to 18% for studies with and without pelvic nodes irradiation, respectively. Chronic GI grade 2+ toxicity rates were between 4% and 50.1% vs. 0% and 40%. SBRT of prostate and positive pelvic nodes only showed similar toxicity rates as SBRT for the prostate only. Among the trials that reported on ADT use, the majority of HR PCA patients underwent ADT for at least 2 months; mostly neoadjuvant and concurrent. Biochemical control rates ranged from 82% to 100% after 2 years and 56% to 100% after 3 years. Only a few studies reported longer follow-up data.
At this point, SBRT with or without pelvic ENI cannot be considered the standard of care in HR PCA, due to missing level 1 evidence. Treatment may be offered to selected patients at specialized centers with access to high-precision RT. While concomitant ADT is the current standard of care, the necessary duration of ADT in combination with SBRT remains unclear. Ideally, all eligible patients should be enrolled in clinical trials.
放射治疗(RT)是局部前列腺癌(PCA)所有风险组合的既定且可能治愈的治疗选择。雄激素剥夺治疗(ADT)和剂量递增的RT可进一步改善高危(HR)PCA的治疗效果。近年来,基于大分割RT的更短RT方案已显示出相同的治疗效果。立体定向体部放疗(SBRT)是一种高度适形的RT技术,可实现超分割放疗,已证明在低危和中危PCA患者中安全有效。关于SBRT在HR PCA中的作用的数据很少。特别是,需要解决盆腔选择性淋巴结照射(ENI)的必要性。因此,我们进行了一项系统评价,以分析关于观察到的毒性、ADT处方实践和肿瘤学结果的现有数据,以更清楚地了解SBRT在HR PCA中的价值。
我们于2020年6月在PubMed和Embase电子数据库中搜索了“前列腺癌”、“立体定向”和“放射治疗”等术语。我们遵循系统评价和Meta分析的首选报告项目(PRISMA)建议。
经过严格的筛选过程,我们确定了18项符合所有选择标准的个体研究进行进一步分析。另外纳入了5项研究,因为它们的内容被认为是相关的。三项试验报告了包括盆腔淋巴结的前列腺SBRT;2项采用ENI,1项仅针对盆腔阳性淋巴结。其余研究仅调查了前列腺的SBRT。在研究盆腔淋巴结照射的研究中,2级及以上急性泌尿生殖系统(GU)毒性在12%至46.7%之间,而仅前列腺研究中的毒性范围为0%至89%。2级及以上慢性GU毒性分别为7%至60%和2%至56.7%。有和没有盆腔淋巴结照射的研究中,急性胃肠道(GI)2级及以上毒性分别为0%至4%和0%至18%。慢性GI 2级及以上毒性率分别为4%至50.1%和0%至40%。仅前列腺和盆腔阳性淋巴结的SBRT显示出与仅前列腺SBRT相似的毒性率。在报告ADT使用情况的试验中,大多数HR PCA患者接受ADT至少2个月;大多为新辅助和同步使用。2年后生化控制率在82%至100%之间,3年后在56%至100%之间。只有少数研究报告了更长时间的随访数据。
目前,由于缺乏一级证据,有或没有盆腔ENI的SBRT不能被视为HR PCA的标准治疗方法。可以在能够进行高精度RT的专业中心为选定的患者提供治疗。虽然同步ADT是目前的标准治疗方法,但ADT与SBRT联合使用的必要持续时间仍不清楚。理想情况下,所有符合条件的患者都应参加临床试验。