Department for Health Evidence, Radboud Institute for Health Sciences, Radboud University Medical Centre, Nijmegen, The Netherlands.
East, Central and Southern Africa Health Community, Arusha, Tanzania.
Int J Health Policy Manag. 2022 Jul 1;11(7):1120-1131. doi: 10.34172/ijhpm.2021.09. Epub 2021 Feb 23.
Access to surgical care is poor in Tanzania. The country is at the implementation stage of its first National Surgical, Obstetric, and Anesthesia Plan (NSOAP; 2018-2025) aiming to scale up surgery. This study aimed to calculate the costs of providing surgical care at the district and regional hospitals.
Two district hospitals (DHs) and the regional referral hospital (RH) in Arusha region were selected. All the staff, buildings, equipment, and medical and non-medical supplies deployed in running the hospitals over a 12 month period were identified and quantified from interviews and hospital records. Using a combination of step-down costing (SDC) and activity-based costing (ABC), all costs attributed to surgeries were established and then distributed over the individual types of surgeries. These costs were delineated into pre-operative, intra-operative, and post-operative components.
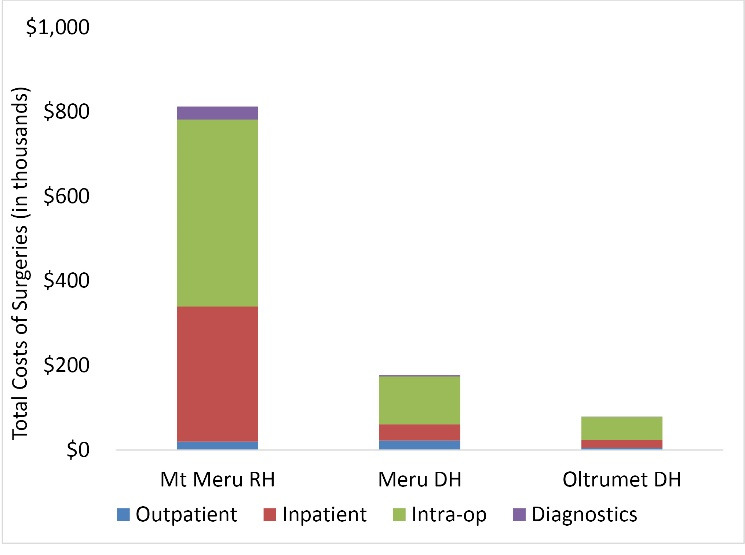
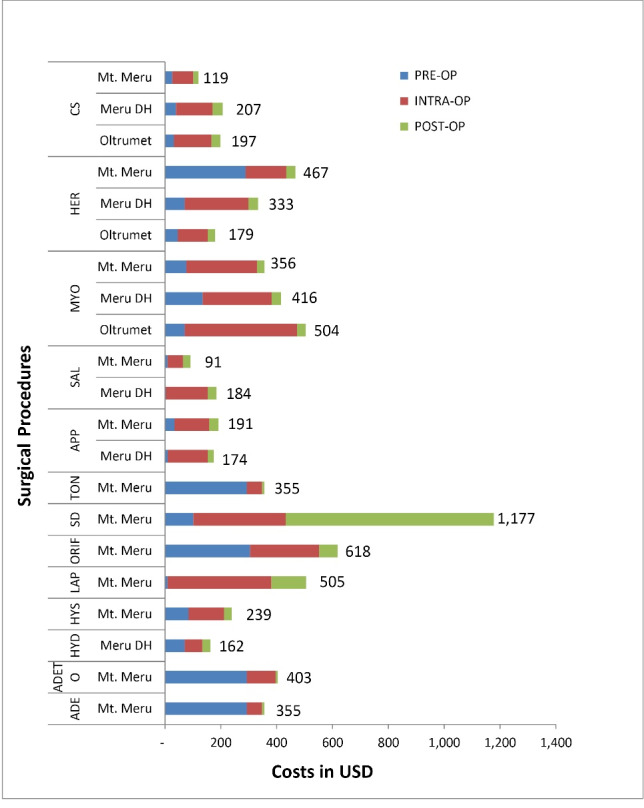
The total annual costs of running the clinical cost centres ranged from $567k at Oltrumet DH to $3453k at Mt Meru RH. The total costs of surgeries ranged from $79k to $813k; amounting to 12%-22% of the total costs of running the hospitals. At least 70% of the costs were salaries. Unit costs and relative shares of capital costs were generally higher at the DHs. Two-thirds of all the procedures incurred at least 60% of their costs in the theatre. Open reduction and internal fixation (ORIF) performed at the regional hospital was cheaper ($618) than surgical debridement (plus conservative treatment) due to prolonged post-operative inpatient care associated with the latter ($1177), but was performed infrequently due mostly to unavailability of implants.
Lower unit costs and shares of capital costs at the RH reflect an advantage of economies of scale and scope at the RH, and a possible underutilization of capacity at the DHs. Greater efficiencies make a case for concentration and scale-up of surgical services at the RHs, but there is a stronger case for scaling up district-level surgeries, not only for equitable access to services, but also to drive down unit costs there, and free up RH resources for more complex cases such as ORIF.
坦桑尼亚的外科护理服务难以获得。该国正处于其首个国家外科、产科和麻醉计划(NSOAP;2018-2025 年)的实施阶段,旨在扩大手术服务规模。本研究旨在计算在地区和区域医院提供外科护理的成本。
选择阿鲁沙地区的 2 家地区医院(DH)和区域转诊医院(RH)。通过访谈和医院记录,确定并量化了在 12 个月期间运行医院所需的所有员工、建筑物、设备以及医疗和非医疗用品。使用逐步降阶成本法(SDC)和基于活动的成本法(ABC)相结合的方法,确定了所有与手术相关的成本,并将其分配到各个手术类型中。这些成本被划分为术前、术中、术后三个部分。
临床成本中心的年运行总成本从 Oltrumet DH 的 56.7 万美元到 Mt Meru RH 的 345.3 万美元不等。手术总成本从 7.9 万美元到 81.3 万美元不等;占医院运行总成本的 12%-22%。至少 70%的成本是工资。DH 的单位成本和资本成本的相对份额通常较高。所有手术中有三分之二以上的手术在手术室中花费了至少 60%的成本。由于后者与术后住院治疗时间较长相关(1177 美元),因此在区域医院进行的切开复位内固定术(ORIF)比清创术(加保守治疗)更便宜(618 美元),但由于缺乏植入物,该手术不太常见。
RH 的较低单位成本和资本成本份额反映了 RH 的规模经济和范围经济的优势,以及 DH 容量的可能未充分利用。更高的效率为 RH 集中和扩大手术服务提供了理由,但更需要扩大地区级手术服务,不仅是为了公平获得服务,还可以降低那里的单位成本,并为 RH 腾出资源,以处理更复杂的病例,如 ORIF。