Mellado-Artigas Ricard, Mujica Luis Eduardo, Ruiz Magda Liliana, Ferreyro Bruno Leonel, Angriman Federico, Arruti Egoitz, Torres Antoni, Barbeta Enric, Villar Jesús, Ferrando Carlos
Department of Anesthesiology and Critical Care, Hospital Clínic, Institut D'investigació August Pi i Sunyer, Villarroel 170, 08025, Barcelona, Spain.
Department of Mathematics, Faculty of Engineering, Universitat Politècnica de Catalunya, Barcelona, Spain.
J Intensive Care. 2021 Mar 5;9(1):23. doi: 10.1186/s40560-021-00538-8.
We aimed to describe the use of high-flow nasal oxygen (HFNO) in patients with COVID-19 acute respiratory failure and factors associated with a shift to invasive mechanical ventilation.
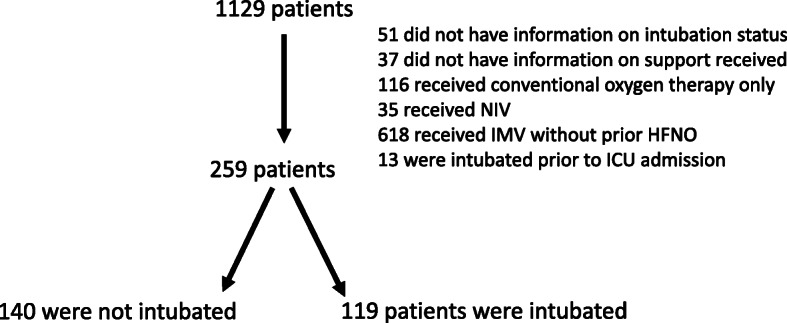
This is a multicenter, observational study from a prospectively collected database of consecutive COVID-19 patients admitted to 36 Spanish and Andorran intensive care units (ICUs) who received HFNO on ICU admission during a 22-week period (March 12-August 13, 2020). Outcomes of interest were factors on the day of ICU admission associated with the need for endotracheal intubation. We used multivariable logistic regression and mixed effects models. A predictive model for endotracheal intubation in patients treated with HFNO was derived and internally validated.
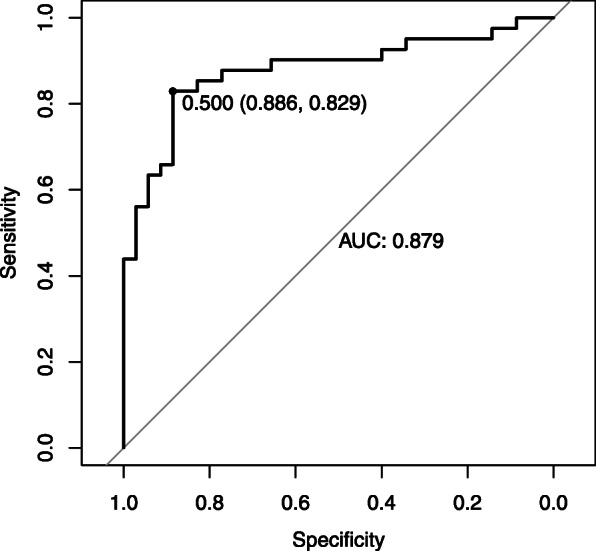
From a total of 259 patients initially treated with HFNO, 140 patients (54%) required invasive mechanical ventilation. Baseline non-respiratory Sequential Organ Failure Assessment (SOFA) score [odds ratio (OR) 1.78; 95% confidence interval (CI) 1.41-2.35], and the ROX index calculated as the ratio of partial pressure of arterial oxygen to inspired oxygen fraction divided by respiratory rate (OR 0.53; 95% CI: 0.37-0.72), and pH (OR 0.47; 95% CI: 0.24-0.86) were associated with intubation. Hospital site explained 1% of the variability in the likelihood of intubation after initial treatment with HFNO. A predictive model including non-respiratory SOFA score and the ROX index showed excellent performance (AUC 0.88, 95% CI 0.80-0.96).
Among adult critically ill patients with COVID-19 initially treated with HFNO, the SOFA score and the ROX index may help to identify patients with higher likelihood of intubation.
我们旨在描述高流量鼻导管给氧(HFNO)在新型冠状病毒肺炎(COVID-19)急性呼吸衰竭患者中的应用情况,以及与转为有创机械通气相关的因素。
这是一项多中心观察性研究,数据来自前瞻性收集的数据库,该数据库涵盖了在22周期间(2020年3月12日至8月13日)入住36家西班牙和安道尔重症监护病房(ICU)且在ICU入院时接受HFNO治疗的连续COVID-19患者。感兴趣的结局是ICU入院当天与气管插管需求相关的因素。我们使用了多变量逻辑回归和混合效应模型。推导并内部验证了接受HFNO治疗患者气管插管的预测模型。
在最初接受HFNO治疗的259例患者中,140例(54%)需要有创机械通气。基线非呼吸序贯器官衰竭评估(SOFA)评分[比值比(OR)1.78;95%置信区间(CI)1.41 - 2.35]、动脉血氧分压与吸入氧分数之比除以呼吸频率计算得出的ROX指数(OR 0.53;95% CI:0.37 - 0.72)以及pH值(OR 0.47;95% CI:0.24 - 0.86)与插管相关。医院地点解释了初始接受HFNO治疗后插管可能性变异性的1%。包含非呼吸SOFA评分和ROX指数的预测模型表现出色(曲线下面积[AUC] 0.88,95% CI 0.80 - 0.96)。
在最初接受HFNO治疗的成年COVID-19危重症患者中,SOFA评分和ROX指数可能有助于识别插管可能性较高的患者。