Assistance Publique-Hôpitaux de Paris, Infectious and Tropical Diseases Department, Bichat-Claude Bernard Hospital, INSERM, IAME, UMR 1137, University of Paris, Paris, France.
Division of Infectious Diseases, Tokyo Metropolitan Tama Medical Center, Tokyo, Japan.
Lancet Respir Med. 2021 May;9(5):522-532. doi: 10.1016/S2213-2600(21)00099-0. Epub 2021 Mar 4.
Elevated proinflammatory cytokines are associated with greater COVID-19 severity. We aimed to assess safety and efficacy of sarilumab, an interleukin-6 receptor inhibitor, in patients with severe (requiring supplemental oxygen by nasal cannula or face mask) or critical (requiring greater supplemental oxygen, mechanical ventilation, or extracorporeal support) COVID-19.
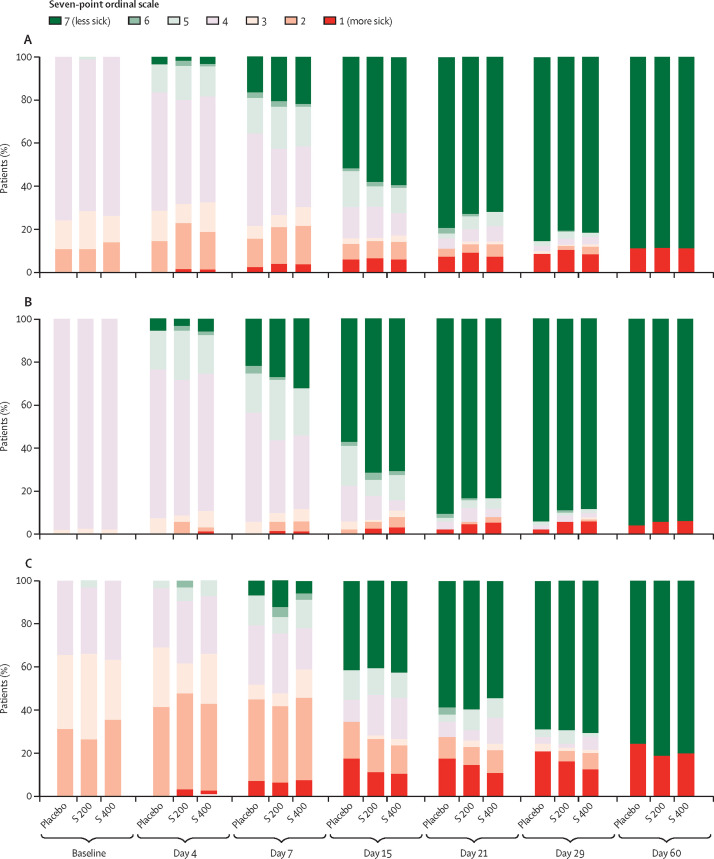
We did a 60-day, randomised, double-blind, placebo-controlled, multinational phase 3 trial at 45 hospitals in Argentina, Brazil, Canada, Chile, France, Germany, Israel, Italy, Japan, Russia, and Spain. We included adults (≥18 years) admitted to hospital with laboratory-confirmed SARS-CoV-2 infection and pneumonia, who required oxygen supplementation or intensive care. Patients were randomly assigned (2:2:1 with permuted blocks of five) to receive intravenous sarilumab 400 mg, sarilumab 200 mg, or placebo. Patients, care providers, outcome assessors, and investigators remained masked to assigned intervention throughout the course of the study. The primary endpoint was time to clinical improvement of two or more points (seven point scale ranging from 1 [death] to 7 [discharged from hospital]) in the modified intention-to-treat population. The key secondary endpoint was proportion of patients alive at day 29. Safety outcomes included adverse events and laboratory assessments. This study is registered with ClinicalTrials.gov, NCT04327388; EudraCT, 2020-001162-12; and WHO, U1111-1249-6021.
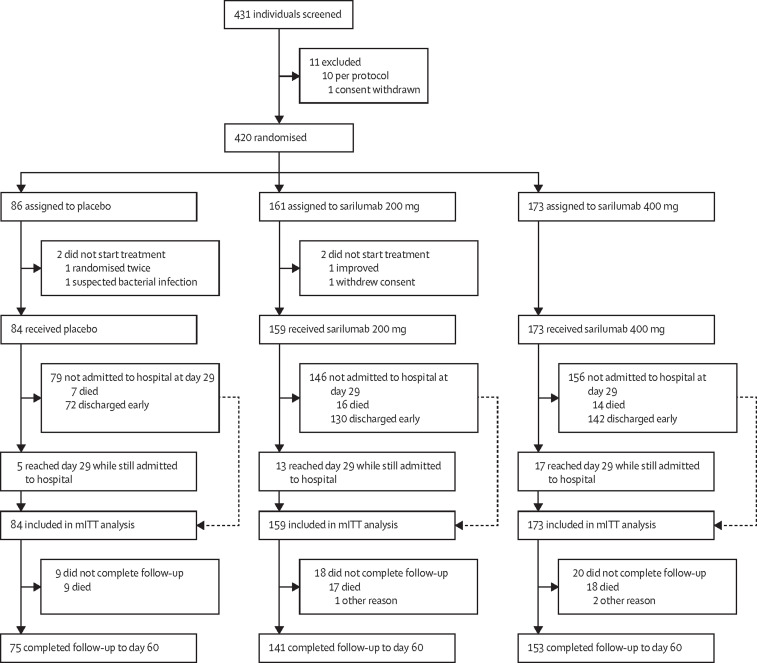
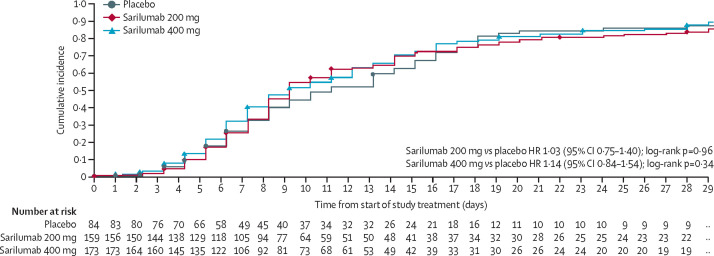
Between March 28 and July 3, 2020, of 431 patients who were screened, 420 patients were randomly assigned and 416 received placebo (n=84 [20%]), sarilumab 200 mg (n=159 [38%]), or sarilumab 400 mg (n=173 [42%]). At day 29, no significant differences were seen in median time to an improvement of two or more points between placebo (12·0 days [95% CI 9·0 to 15·0]) and sarilumab 200 mg (10·0 days [9·0 to 12·0]; hazard ratio [HR] 1·03 [95% CI 0·75 to 1·40]; log-rank p=0·96) or sarilumab 400 mg (10·0 days [9·0 to 13·0]; HR 1·14 [95% CI 0·84 to 1·54]; log-rank p=0·34), or in proportions of patients alive (77 [92%] of 84 patients in the placebo group; 143 [90%] of 159 patients in the sarilumab 200 mg group; difference -1·7 [-9·3 to 5·8]; p=0·63 vs placebo; and 159 [92%] of 173 patients in the sarilumab 400 mg group; difference 0·2 [-6·9 to 7·4]; p=0·85 vs placebo). At day 29, there were numerical, non-significant survival differences between sarilumab 400 mg (88%) and placebo (79%; difference +8·9% [95% CI -7·7 to 25·5]; p=0·25) for patients who had critical disease. No unexpected safety signals were seen. The rates of treatment-emergent adverse events were 65% (55 of 84) in the placebo group, 65% (103 of 159) in the sarilumab 200 mg group, and 70% (121 of 173) in the sarilumab 400 mg group, and of those leading to death 11% (nine of 84) were in the placebo group, 11% (17 of 159) were in the sarilumab 200 mg group, and 10% (18 of 173) were in the sarilumab 400 mg group.
This trial did not show efficacy of sarilumab in patients admitted to hospital with COVID-19 and receiving supplemental oxygen. Adequately powered trials of targeted immunomodulatory therapies assessing survival as a primary endpoint are suggested in patients with critical COVID-19.
Sanofi and Regeneron Pharmaceuticals.
升高的促炎细胞因子与更严重的 COVID-19 严重程度相关。我们旨在评估白细胞介素-6 受体抑制剂沙利鲁单抗在严重(需要通过鼻导管或面罩补充氧气)或危急(需要更大的补充氧气、机械通气或体外支持)COVID-19 患者中的安全性和疗效。
我们在阿根廷、巴西、加拿大、智利、法国、德国、以色列、意大利、日本、俄罗斯和西班牙的 45 家医院进行了一项为期 60 天、随机、双盲、安慰剂对照、多国 3 期试验。我们纳入了因实验室确诊的 SARS-CoV-2 感染和肺炎而住院、需要补充氧气或重症监护的成年人(≥18 岁)。患者被随机分配(2:2:1,使用 5 个区组的随机化置换)接受静脉注射沙利鲁单抗 400mg、沙利鲁单抗 200mg 或安慰剂。在整个研究过程中,患者、护理提供者、结局评估者和研究者对分配的干预措施均保持盲态。主要终点是改良意向治疗人群中达到 2 分或 2 分以上(评分范围为 1 [死亡] 至 7 [出院])的临床改善时间。关键次要终点是第 29 天存活患者的比例。安全性结局包括不良事件和实验室评估。这项研究在 ClinicalTrials.gov、EudraCT 和世卫组织注册,注册号分别为 NCT04327388、2020-001162-12 和 U1111-1249-6021。
在 2020 年 3 月 28 日至 7 月 3 日期间,在筛选的 431 名患者中,420 名患者被随机分配,416 名患者接受安慰剂(n=84 [20%])、沙利鲁单抗 200mg(n=159 [38%])或沙利鲁单抗 400mg(n=173 [42%])。在第 29 天,与安慰剂组(中位时间 12.0 天 [95%CI 9.0 至 15.0])相比,沙利鲁单抗 200mg 组(中位时间 10.0 天 [95%CI 9.0 至 12.0];风险比 [HR] 1.03 [95%CI 0.75 至 1.40];对数秩检验 p=0.96)或沙利鲁单抗 400mg 组(中位时间 10.0 天 [95%CI 9.0 至 13.0];HR 1.14 [95%CI 0.84 至 1.54];对数秩检验 p=0.34)之间,或在第 29 天存活患者的比例方面,没有显著差异。安慰剂组有 77 名(84 名患者中的 92%)、沙利鲁单抗 200mg 组有 143 名(159 名患者中的 90%)、沙利鲁单抗 400mg 组有 159 名(173 名患者中的 92%)存活。差异分别为 -1.7 [-9.3 至 5.8];p=0.63 与安慰剂;沙利鲁单抗 400mg 组存活患者的比例比安慰剂组高 0.2%(差异 6.9 至 7.4;p=0.85)。在第 29 天,与安慰剂相比,沙利鲁单抗 400mg 组(88%)的死亡率比安慰剂组(79%)高 8.9%(差异+8.9% [95%CI 7.7 至 25.5];p=0.25),这一差异在患有危急疾病的患者中更为明显。未发现新的安全性信号。安慰剂组、沙利鲁单抗 200mg 组和沙利鲁单抗 400mg 组治疗出现的不良事件发生率分别为 65%(55/84)、65%(103/159)和 70%(121/173),导致死亡的发生率分别为 11%(9/84)、11%(17/159)和 10%(18/173)。
这项试验没有显示沙利鲁单抗在接受补充氧气治疗的 COVID-19 住院患者中的疗效。建议在患有危急 COVID-19 的患者中进行更有力的靶向免疫调节疗法试验,以生存为主要终点。
赛诺菲和再生元制药公司。