Department of Pharmacy & Pharmacology, Antoni van Leeuwenhoek Hospital/Netherlands Cancer Institute, Amsterdam, The Netherlands.
Drugs for Neglected Diseases Initiative, Geneva, Switzerland.
J Antimicrob Chemother. 2021 Apr 13;76(5):1258-1268. doi: 10.1093/jac/dkab013.
Despite high HIV co-infection prevalence in Ethiopian visceral leishmaniasis (VL) patients, the adequacy of antileishmanial drug exposure in this population and effect of HIV-VL co-morbidity on pharmacokinetics of antileishmanial and antiretroviral (ARV) drugs is still unknown.
HIV-VL co-infected patients received the recommended liposomal amphotericin B (LAmB) monotherapy (total dose 40 mg/kg over 24 days) or combination therapy of LAmB (total dose 30 mg/kg over 11 days) plus 28 days 100 mg/day miltefosine, with possibility to extend treatment for another cycle. Miltefosine, total amphotericin B and ARV concentrations were determined in dried blood spots or plasma using LC-MS/MS.
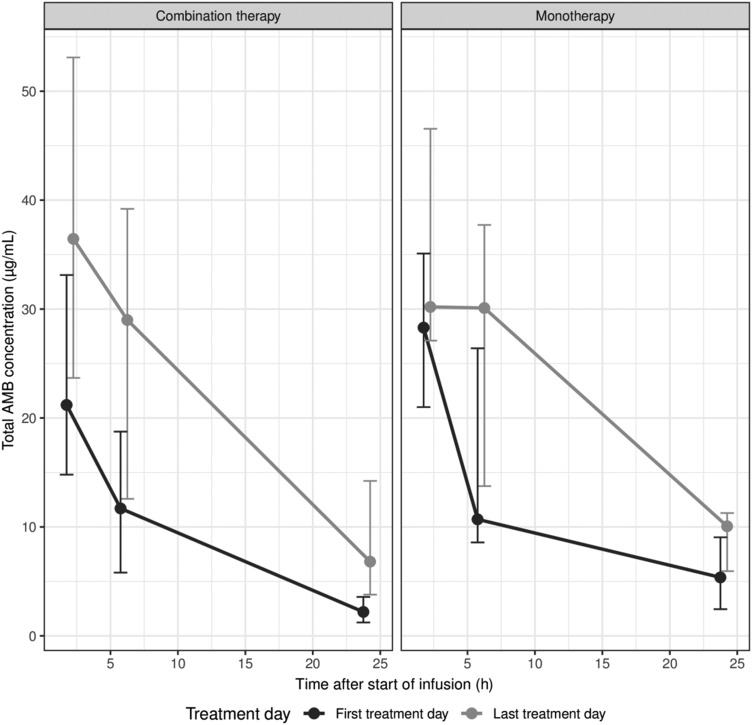
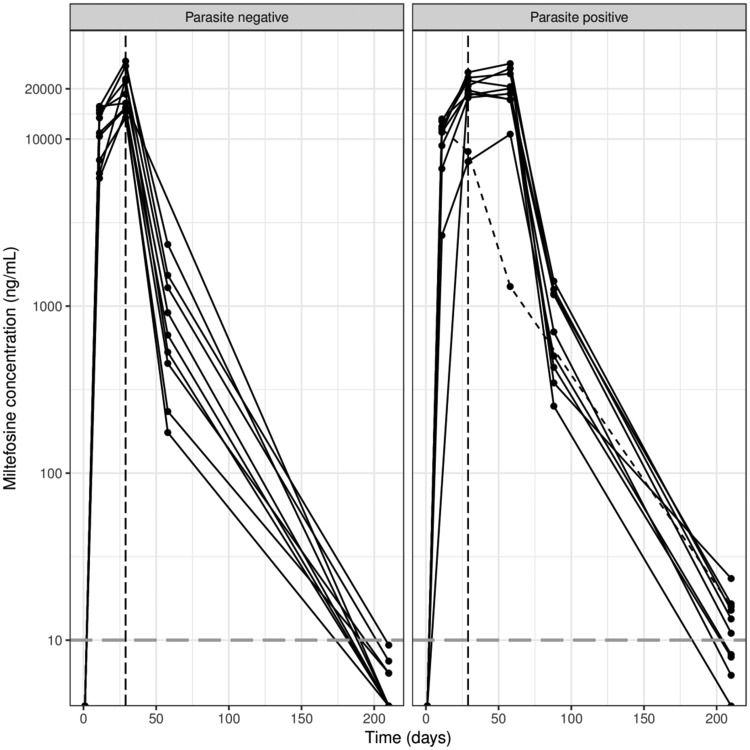
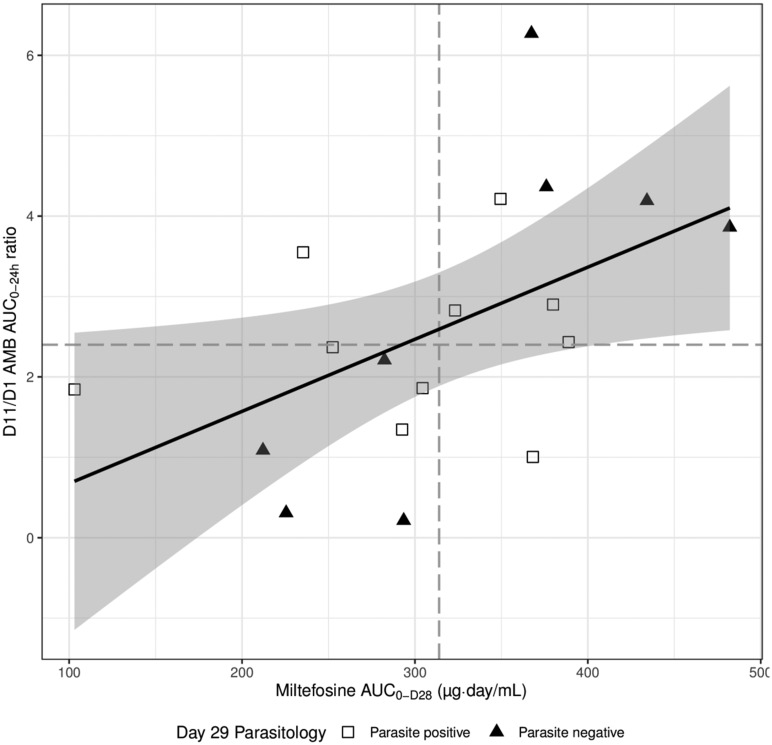
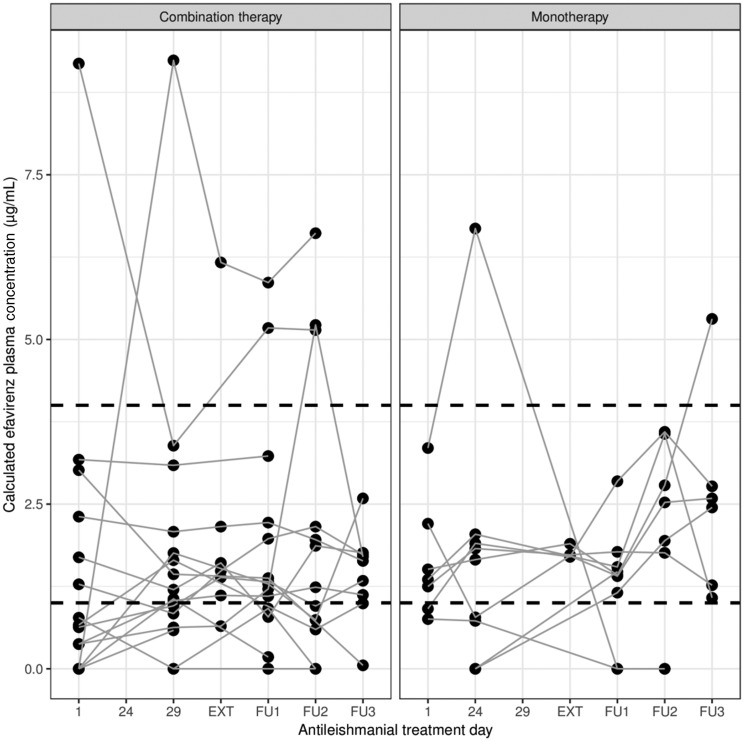
Median (IQR) amphotericin B Cmax on Day 1 was 24.6 μg/mL (17.0-34.9 μg/mL), which increased to 40.9 (25.4-53.1) and 33.2 (29.0-46.6) μg/mL on the last day of combination and monotherapy, respectively. Day 28 miltefosine concentration was 18.7 (15.4-22.5) μg/mL. Miltefosine exposure correlated with amphotericin B accumulation. ARV concentrations were generally stable during antileishmanial treatment, although efavirenz Cmin was below the 1 μg/mL therapeutic target for many patients.
This study demonstrates that antileishmanial drug exposure was low in this cohort of HIV co-infected VL patients. Amphotericin B Cmax was 2-fold lower than previously observed in non-VL patients. Miltefosine exposure in HIV-VL co-infected patients was 35% lower compared with adult VL patients in Eastern Africa, only partially explained by a 19% lower dose, possibly warranting a dose adjustment. Adequate drug exposure in these HIV-VL co-infected patients is especially important given the high proportion of relapses.
尽管埃塞俄比亚内脏利什曼病(VL)患者中 HIV 合并感染率较高,但该人群中抗利什曼药物的暴露程度以及 HIV-VL 合并感染对抗利什曼和抗逆转录病毒(ARV)药物药代动力学的影响尚不清楚。
HIV-VL 合并感染患者接受了推荐的脂质体两性霉素 B(LAmB)单药治疗(总剂量为 40mg/kg,分 24 天给予)或 LAmB 联合治疗(总剂量为 30mg/kg,分 11 天给予)加 28 天 100mg/天米替福新,如有必要可延长一个疗程。使用 LC-MS/MS 在干血斑或血浆中测定米替福新、总两性霉素 B 和 ARV 浓度。
第 1 天两性霉素 B Cmax 的中位数(IQR)为 24.6μg/mL(17.0-34.9μg/mL),在联合和单药治疗的最后一天分别增加到 40.9(25.4-53.1)和 33.2(29.0-46.6)μg/mL。第 28 天米替福新浓度为 18.7(15.4-22.5)μg/mL。米替福新暴露与两性霉素 B 积累相关。在抗利什曼病治疗期间,ARV 浓度通常保持稳定,尽管许多患者的依非韦伦 Cmin 低于 1μg/mL 的治疗目标。
本研究表明,HIV 合并感染 VL 患者的抗利什曼药物暴露水平较低。两性霉素 B Cmax 比之前在非 VL 患者中观察到的低 2 倍。与东非的成人 VL 患者相比,HIV-VL 合并感染患者的米替福新暴露水平低 35%,部分原因是剂量降低 19%,可能需要调整剂量。鉴于较高的复发率,这些 HIV-VL 合并感染患者获得充分的药物暴露尤为重要。