Otorhinolaryngology Service, Hospital de Especialidades, Centro Médico Nacional Siglo XXI, Instituto Mexicano del Seguro Social, Mexico City, Mexico.
Emergency Department. Hospital de Especialidades, Centro Médico Nacional Siglo XXI, Instituto Mexicano del Seguro Social, Mexico City, Mexico.
BMC Infect Dis. 2021 Mar 11;21(1):255. doi: 10.1186/s12879-021-05930-1.
The SARS-CoV-2 pandemic continues to be a priority health problem; According to the World Health Organization data from October 13, 2020, 37,704,153 confirmed COVID-19 cases have been reported, including 1,079,029 deaths, since the outbreak. The identification of potential symptoms has been reported to be a useful tool for clinical decision-making in emergency departments to avoid overload and improve the quality of care. The aim of this study was to evaluate the performances of symptoms as a diagnostic tool for SARS -CoV-2 infection.
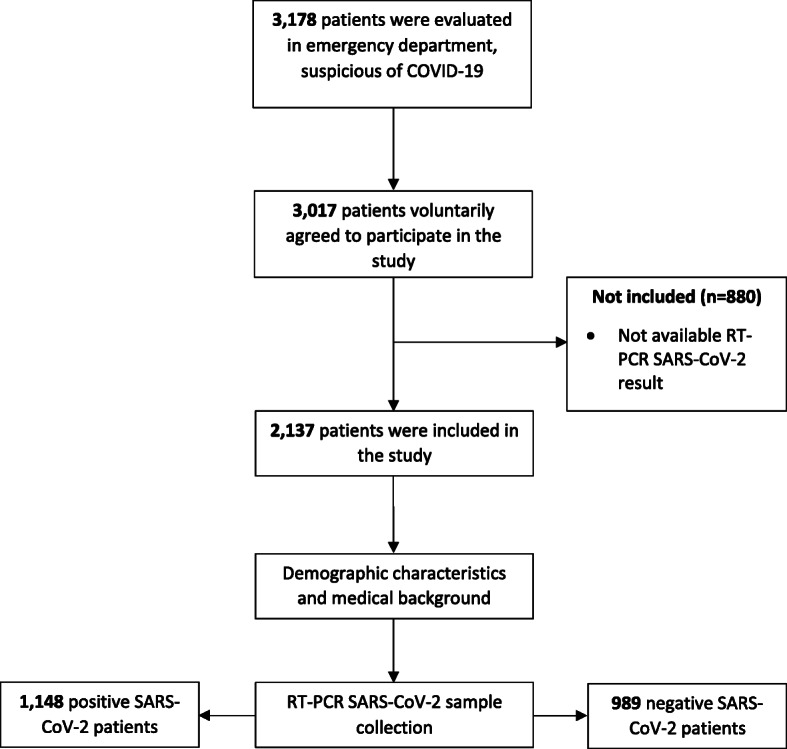
An observational, cross-sectional, prospective and analytical study was carried out, during the period of time from April 14 to July 21, 2020. Data (demographic variables, medical history, respiratory and non-respiratory symptoms) were collected by emergency physicians. The diagnosis of COVID-19 was made using SARS-CoV-2 RT-PCR. The diagnostic accuracy of these characteristics for COVID-19 was evaluated by calculating the positive and negative likelihood ratios. A Mantel-Haenszel and multivariate logistic regression analysis was performed to assess the association of symptoms with COVID-19.
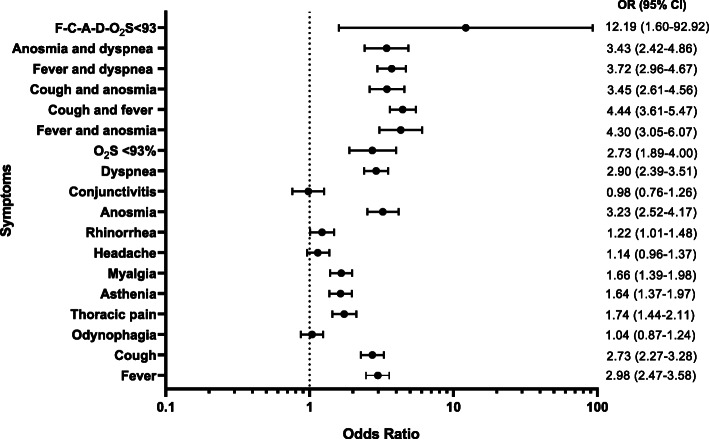
A prevalence of 53.72% of SARS-CoV-2 infection was observed. The symptom with the highest sensitivity was cough 71%, and a specificity of 52.68%. The symptomatological scale, constructed from 6 symptoms, obtained a sensitivity of 83.45% and a specificity of 32.86%, taking ≥2 symptoms as a cut-off point. The symptoms with the greatest association with SARS-CoV-2 were: anosmia odds ratio (OR) 3.2 (95% CI; 2.52-4.17), fever OR 2.98 (95% CI; 2.47-3.58), dyspnea OR 2.9 (95% CI; 2.39-3.51]) and cough OR 2.73 (95% CI: 2.27-3.28).
The combination of ≥2 symptoms / signs (fever, cough, anosmia, dyspnea and oxygen saturation < 93%, and headache) results in a highly sensitivity model for a quick and accurate diagnosis of COVID-19, and should be used in the absence of ancillary diagnostic studies. Symptomatology, alone and in combination, may be an appropriate strategy to use in the emergency department to guide the behaviors to respond to the disease.
Institutional registration R-2020-3601-145, Federal Commission for the Protection against Sanitary Risks 17 CI-09-015-034, National Bioethics Commission: 09 CEI-023-2017082 .
SARS-CoV-2 大流行仍然是一个优先的健康问题;根据世界卫生组织 2020 年 10 月 13 日的数据,自疫情爆发以来,已报告 37704130 例确诊的 COVID-19 病例,包括 1079029 例死亡。据报道,确定潜在症状是急诊科临床决策的有用工具,可避免超负荷并提高护理质量。本研究旨在评估症状作为 SARS-CoV-2 感染诊断工具的性能。
这是一项观察性、横断面、前瞻性和分析性研究,于 2020 年 4 月 14 日至 7 月 21 日期间进行。急诊医师收集数据(人口统计学变量、病史、呼吸和非呼吸症状)。使用 SARS-CoV-2 RT-PCR 进行 COVID-19 的诊断。通过计算阳性和阴性似然比来评估这些特征对 COVID-19 的诊断准确性。采用 Mantel-Haenszel 和多变量逻辑回归分析评估症状与 COVID-19 的关联。
观察到 SARS-CoV-2 感染的流行率为 53.72%。敏感性最高的症状是咳嗽 71%,特异性为 52.68%。从 6 种症状构建的症状量表的敏感性为 83.45%,特异性为 32.86%,以≥2 种症状作为截断值。与 SARS-CoV-2 相关性最大的症状为:嗅觉丧失的比值比(OR)3.2(95%CI;2.52-4.17),发热 OR 2.98(95%CI;2.47-3.58),呼吸困难 OR 2.9(95%CI;2.39-3.51)]和咳嗽 OR 2.73(95%CI:2.27-3.28)。
≥2 种症状/体征(发热、咳嗽、嗅觉丧失、呼吸困难和血氧饱和度 < 93%,头痛)的组合可快速准确诊断 COVID-19,应在缺乏辅助诊断研究的情况下使用。单独使用和组合使用症状可能是急诊科指导应对疾病行为的一种合适策略。
机构注册 R-2020-3601-145,联邦保护卫生风险委员会 17 CI-09-015-034,国家生物伦理委员会:09 CEI-023-2017082 。