Health System and Reproductive Health Research Directorate, Ethiopian Public Health Institute, Addis Ababa, Ethiopia.
College of Medicine and Health Sciences, Institute of Public Health, University of Gondar, Gondar, Ethiopia.
PLoS One. 2021 Mar 12;16(3):e0247474. doi: 10.1371/journal.pone.0247474. eCollection 2021.
Due to low care utilization, a complex intervention was done for two years to optimize the Ethiopian Health Extension Program. Improved quality of the integrated community case management services was an intermediate outcome of this intervention through community education and mobilization, capacity building of health workers, and strengthening of district ownership and accountability of sick child services. We evaluated the association between the intervention and the health extension workers' ability to correctly classify common childhood illnesses in four regions of Ethiopia.
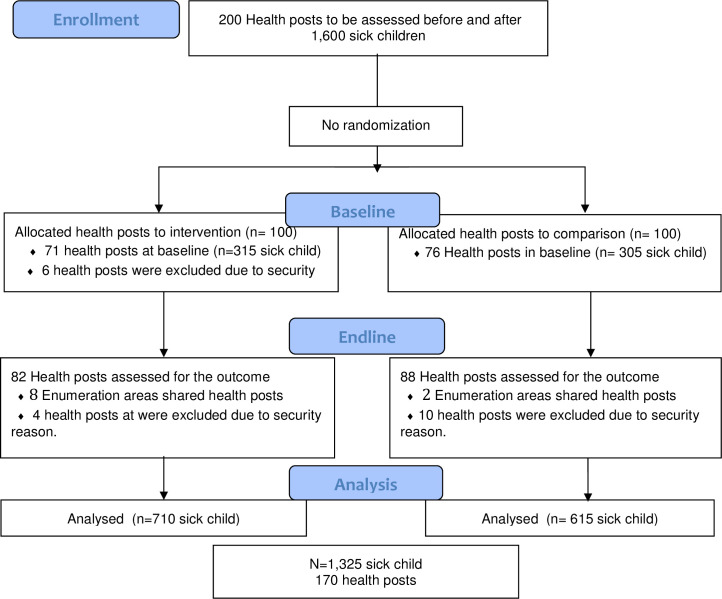
Baseline and endline assessments were done in 2016 and 2018 in intervention and comparison areas in four regions of Ethiopia. Ill children aged 2 to 59 months were mobilized to visit health posts for an assessment that was followed by re-examination. We analyzed sensitivity, specificity, and difference-in-difference of correct classification with multilevel mixed logistic regression in intervention and comparison areas at baseline and endline.
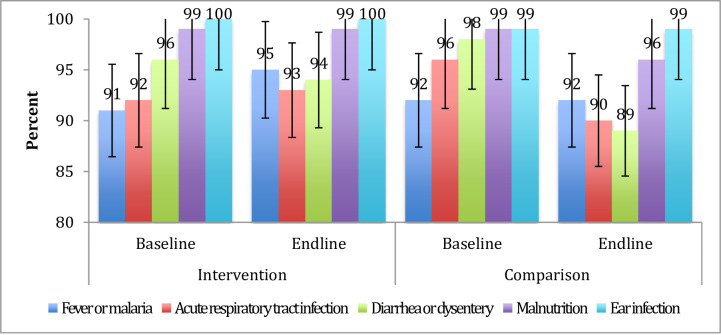
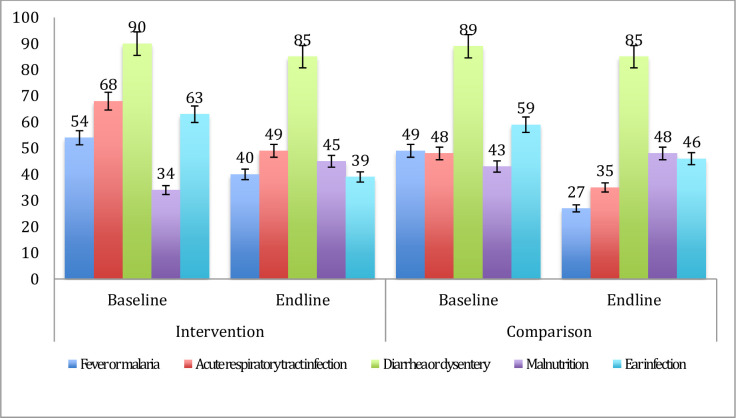
Health extensions workers' consultations with ill children were observed in intervention (n = 710) and comparison areas (n = 615). At baseline, re-examination of the children showed that in intervention areas, health extension workers' sensitivity for fever or malaria was 54%, 68% for respiratory infections, 90% for diarrheal diseases, and 34% for malnutrition. At endline, it was 40% for fever or malaria, 49% for respiratory infections, 85% for diarrheal diseases, and 48% for malnutrition. Specificity was higher (89-100%) for all childhood illnesses. Difference-in-differences was 6% for correct classification of fever or malaria [aOR = 1.45 95% CI: 0.81-2.60], 4% for respiratory tract infection [aOR = 1.49 95% CI: 0.81-2.74], and 5% for diarrheal diseases [aOR = 1.74 95% CI: 0.77-3.92].
This study revealed that the Optimization of Health Extension Program intervention, which included training, supportive supervision, and performance reviews of health extension workers, was not associated with an improved classification of childhood illnesses by these Ethiopian primary health care workers.
ISRCTN12040912, http://www.isrctn.com/ISRCTN12040912.
由于利用率低,对埃塞俄比亚卫生延伸计划进行了为期两年的复杂干预,以优化其服务。通过社区教育和动员、卫生工作者能力建设以及加强地区对患病儿童服务的所有权和问责制,提高综合社区病例管理服务的质量是该干预的一个中期结果。我们评估了干预措施与埃塞俄比亚四个地区卫生推广工作者正确分类常见儿童疾病的能力之间的关系。
2016 年和 2018 年在埃塞俄比亚四个地区的干预和对照地区进行了基线和终线评估。动员 2 至 59 个月大的患病儿童前往卫生所进行评估,随后进行复查。我们在基线和终线时使用多水平混合逻辑回归分析了干预区和对照区的正确分类的敏感性、特异性和差异。
在干预区(n=710)和对照区(n=615)观察到卫生推广工作者与患病儿童的咨询。在基线时,对儿童的复查显示,在干预区,卫生推广工作者对发热或疟疾的敏感性为 54%,对呼吸道感染的敏感性为 68%,对腹泻病的敏感性为 90%,对营养不良的敏感性为 34%。在终线时,发热或疟疾的敏感性为 40%,呼吸道感染的敏感性为 49%,腹泻病的敏感性为 85%,营养不良的敏感性为 48%。所有儿童疾病的特异性均较高(89-100%)。差异在分类发热或疟疾方面为 6%[优势比(aOR)=1.45,95%置信区间(CI):0.81-2.60],在分类呼吸道感染方面为 4%[aOR=1.49,95%CI:0.81-2.74],在分类腹泻病方面为 5%[aOR=1.74,95%CI:0.77-3.92]。
本研究表明,包括培训、支持性监督和对卫生推广工作者的绩效评估在内的埃塞俄比亚初级卫生保健工作者对卫生延伸计划的优化干预,并未改善这些工作者对儿童疾病的分类。
ISRCTN8332235,http://www.isrctn.com/ISRCTN8332235。