García-Villalba Manuel, Rossini Lorenzo, Gonzalo Alejandro, Vigneault Davis, Martinez-Legazpi Pablo, Durán Eduardo, Flores Oscar, Bermejo Javier, McVeigh Elliot, Kahn Andrew M, Del Álamo Juan C
Bioengineering and Aerospace Engineering Department, Carlos III University of Madrid, Leganés, Spain.
Department of Mechanical and Aerospace Engineering, University of California, San Diego, La Jolla, CA, United States.
Front Physiol. 2021 Feb 26;12:596596. doi: 10.3389/fphys.2021.596596. eCollection 2021.
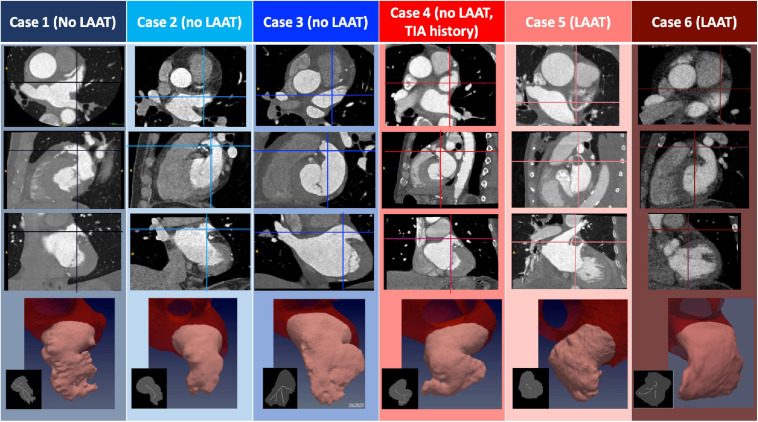
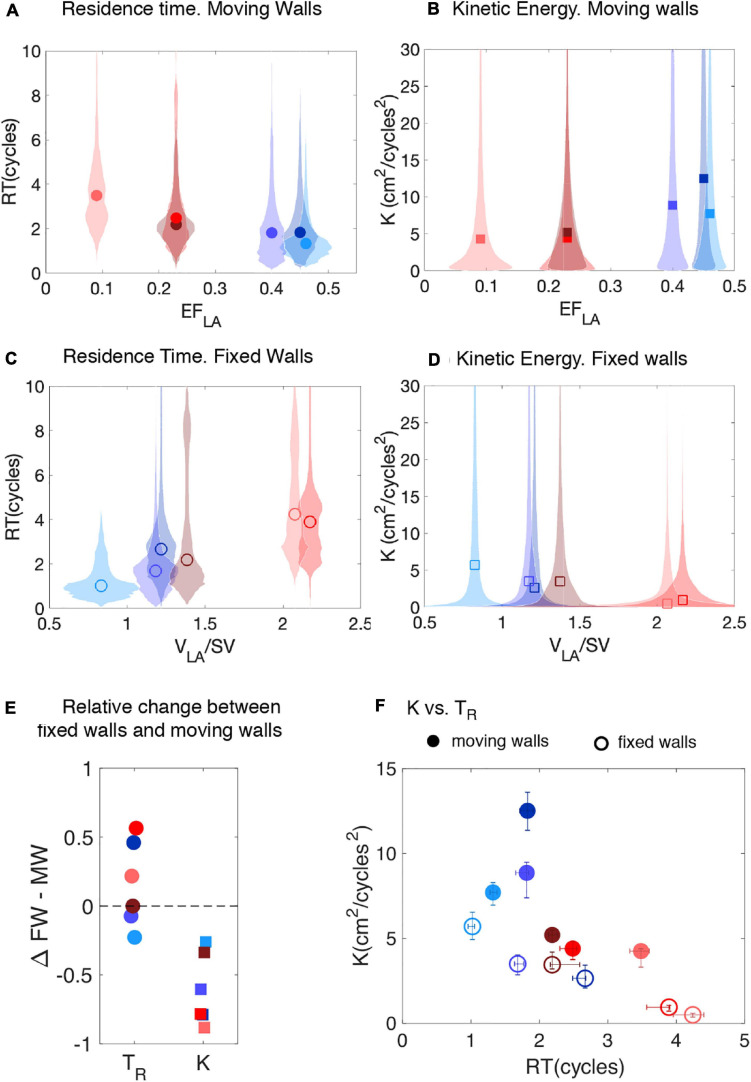
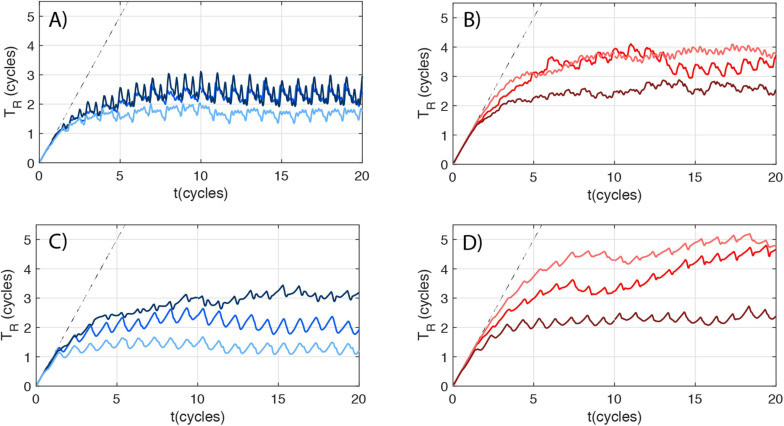
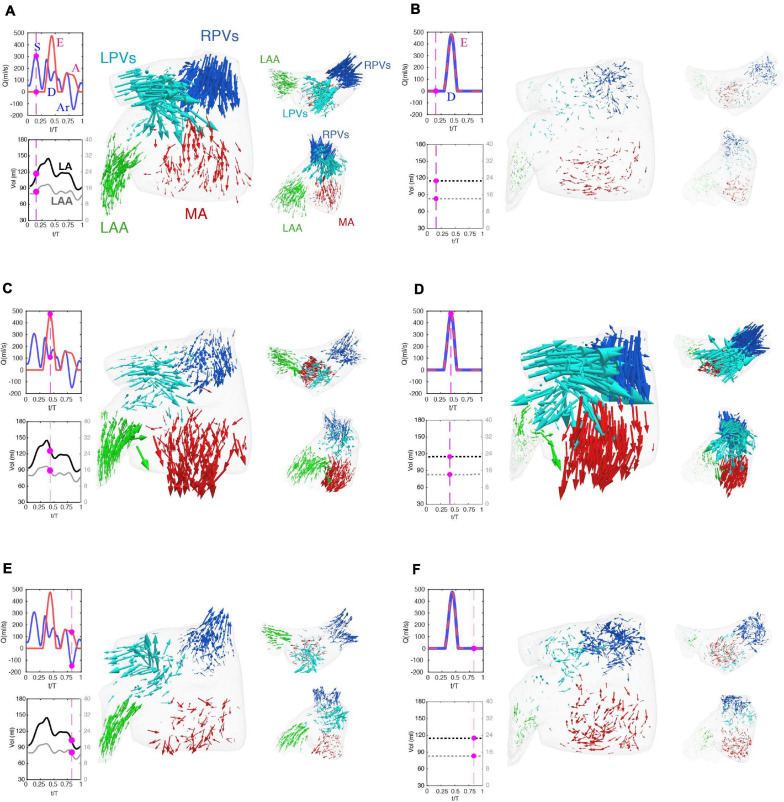
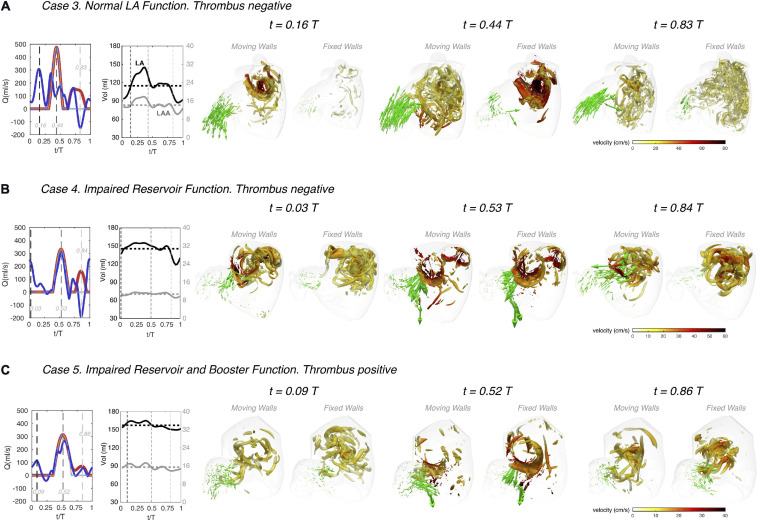
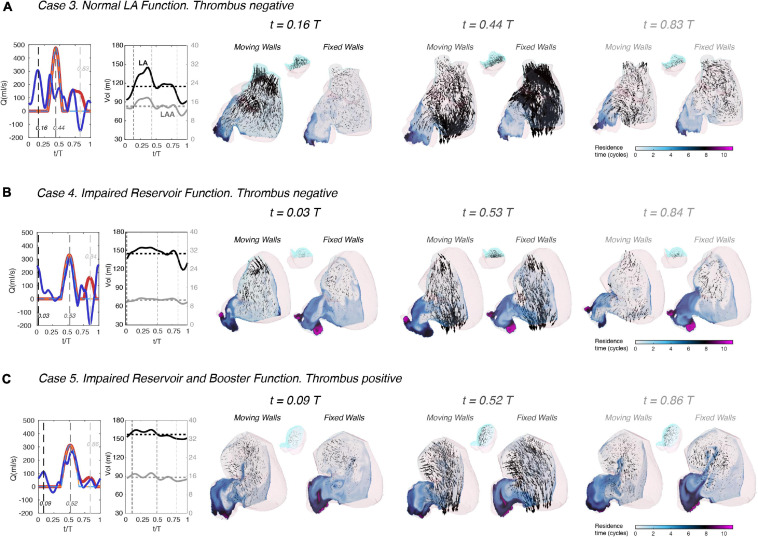
Atrial fibrillation (AF) alters left atrial (LA) hemodynamics, which can lead to thrombosis in the left atrial appendage (LAA), systemic embolism and stroke. A personalized risk-stratification of AF patients for stroke would permit improved balancing of preventive anticoagulation therapies against bleeding risk. We investigated how LA anatomy and function impact LA and LAA hemodynamics, and explored whether patient-specific analysis by computational fluid dynamics (CFD) can predict the risk of LAA thrombosis. We analyzed 4D-CT acquisitions of LA wall motion with an in-house immersed-boundary CFD solver. We considered six patients with diverse atrial function, three with either a LAA thrombus (removed digitally before running the simulations) or a history of transient ischemic attacks (LAAT/TIA-pos), and three without a LAA thrombus or TIA (LAAT/TIA-neg). We found that blood inside the left atrial appendage of LAAT/TIA-pos patients had marked alterations in residence time and kinetic energy when compared with LAAT/TIA-neg patients. In addition, we showed how the LA conduit, reservoir and booster functions distinctly affect LA and LAA hemodynamics. Finally, fixed-wall and moving-wall simulations produced different LA hemodynamics and residence time predictions for each patient. Consequently, fixed-wall simulations risk-stratified our small cohort for LAA thrombosis worse than moving-wall simulations, particularly patients with intermediate LAA residence time. Overall, these results suggest that both wall kinetics and LAA morphology contribute to LAA blood stasis and thrombosis.
心房颤动(AF)会改变左心房(LA)的血流动力学,进而导致左心耳(LAA)血栓形成、全身栓塞和中风。对房颤患者进行个性化的中风风险分层,有助于更好地平衡预防性抗凝治疗与出血风险。我们研究了左心房的解剖结构和功能如何影响左心房和左心耳的血流动力学,并探讨通过计算流体动力学(CFD)进行患者特异性分析是否能够预测左心耳血栓形成的风险。我们使用内部浸入边界CFD求解器分析了左心房壁运动的4D-CT图像。我们纳入了6名心房功能各异的患者,其中3名患有左心耳血栓(在运行模拟之前通过数字方式移除)或有短暂性脑缺血发作病史(LAAT/TIA阳性),另外3名既没有左心耳血栓也没有短暂性脑缺血发作(LAAT/TIA阴性)。我们发现,与LAAT/TIA阴性患者相比,LAAT/TIA阳性患者左心耳内的血液在停留时间和动能方面有明显改变。此外,我们还展示了左心房的管道、储器和助力功能如何分别影响左心房和左心耳的血流动力学。最后,固定壁和移动壁模拟对每位患者产生了不同的左心房血流动力学和停留时间预测结果。因此,固定壁模拟对我们的小队列左心耳血栓形成风险分层的效果不如移动壁模拟,尤其是对于左心耳停留时间中等的患者。总体而言,这些结果表明,壁动力学和左心耳形态均有助于左心耳血液淤滞和血栓形成。