Department of Pathology, Peking Union Medical College Hospital, Molecular Pathology Research Center, Chinese Academy of Medical Sciences, Beijing, China.
Department of Breast Surgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing, China.
Front Immunol. 2021 Feb 24;12:561793. doi: 10.3389/fimmu.2021.561793. eCollection 2021.
Poor response to immune checkpoint inhibitors (ICIs) has been observed in most triple-negative breast cancer (TNBC) cases (around 80%). Our aim was to investigate the status of mismatch repair (MMR), microsatellite instability (MSI), programmed death-ligand 1 (PD-L1), and lymphocyte-activation gene 3 (LAG-3) in TNBC.
A total of 74 TNBC samples were retrospectively analyzed. MMR and MSI were evaluated by immunohistochemistry (IHC) and polymerase chain reaction (PCR) using Promega 1.2 and NCI panels, respectively. PD-L1, LAG-3, and CD8 expression was assessed by IHC.
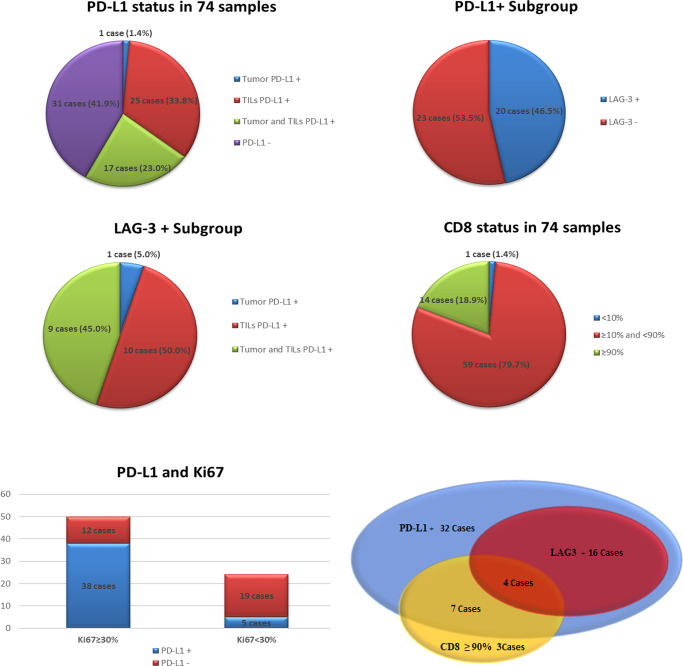
None of the cases demonstrated deficient MMR (dMMR) or MSI. In total, 43/74 cases (58.1%) were PD-L1+, including 1 tumor PD-L1+, 25 tumor-infiltrating lymphocytes (TILs) PD-L1+, and 17 cases involving concurrence of tumor and TIL PD-L1+. The rate of TIL PD-L1+ was remarkably higher than that of tumor PD-L1+ (P<0.001). We identified 20 LAG-3+ cases (27.0%, 20/74), all of which were PD-L1+. Co-expression of PD-L1 and LAG-3 was noted in 46.5% (20/43) of the PD-L1+ population. In the LAG-3+ subtype (co-expression of PD-L1 and LAG-3), high correlation between TILs PD-L1+ and LAG-3+ was observed (P<0.01). A high frequency of CD8+ (98.6%, 73/74) was observed.
dMMR/MSI characteristics may not be a practical predictive marker for ICIs in TNBC. PD-L1+ is more common in TILs than in tumors. In the PD-L1+ population, approximately half of the cases showed LAG-3 co-expression. For patients with a poor response to PD-1(L1) mono ICI, dual blockade of PD-1(L1) and LAG-3 may be a viable option for the management of TNBC.
在大多数三阴性乳腺癌(TNBC)病例(约 80%)中,免疫检查点抑制剂(ICIs)的反应较差。我们的目的是研究 TNBC 中错配修复(MMR)、微卫星不稳定性(MSI)、程序性死亡配体 1(PD-L1)和淋巴细胞激活基因 3(LAG-3)的状态。
回顾性分析了 74 例 TNBC 样本。采用 Promega 1.2 和 NCI 试剂盒通过免疫组化(IHC)和聚合酶链反应(PCR)评估 MMR 和 MSI。通过 IHC 评估 PD-L1、LAG-3 和 CD8 的表达。
无病例表现出 MMR 缺陷(dMMR)或 MSI。共有 43/74 例(58.1%)为 PD-L1+,包括 1 例肿瘤 PD-L1+、25 例肿瘤浸润淋巴细胞(TIL)PD-L1+和 17 例肿瘤和 TIL PD-L1+并存。TIL PD-L1+的发生率明显高于肿瘤 PD-L1+(P<0.001)。我们鉴定出 20 例 LAG-3+病例(27.0%,20/74),均为 PD-L1+。在 PD-L1+人群中,有 46.5%(20/43)存在 PD-L1 和 LAG-3 的共表达。在 LAG-3+亚型(PD-L1 和 LAG-3 的共表达)中,观察到 TILs PD-L1+和 LAG-3+之间高度相关(P<0.01)。CD8+的频率很高(98.6%,74/74)。
dMMR/MSI 特征可能不是 TNBC 中 ICIs 的实用预测标志物。PD-L1+在 TILs 中比在肿瘤中更为常见。在 PD-L1+人群中,约有一半的病例存在 LAG-3 共表达。对于对 PD-1(L1)单药 ICI 反应不佳的患者,PD-1(L1)和 LAG-3 的双重阻断可能是治疗 TNBC 的一种可行选择。