Liu Zhichao, Zhang Xiaobin, Li Bin, Jiang Haoyao, Yang Yang, Hua Rong, Sun Yifeng, Li Zhigang
Department of Thoracic Surgery, Section of Esophageal Surgery, Shanghai Chest Hospital, Shanghai Jiao Tong University, Shanghai, China.
J Thorac Dis. 2021 Feb;13(2):870-882. doi: 10.21037/jtd-20-2347.
The survival benefit of primary tumor surgery for metastatic esophageal cancer (mEC) patients has been observed, but methods for discriminating which individual patients would benefit from surgery have been poorly defined. Herein, a predictive model was developed to test the hypothesis that only certain metastatic patients would gain a survival benefit from primary tumor surgery.
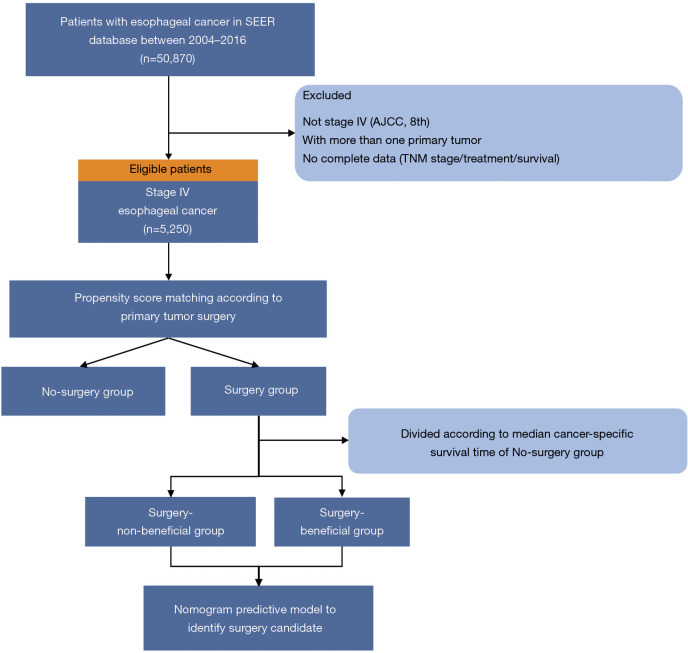
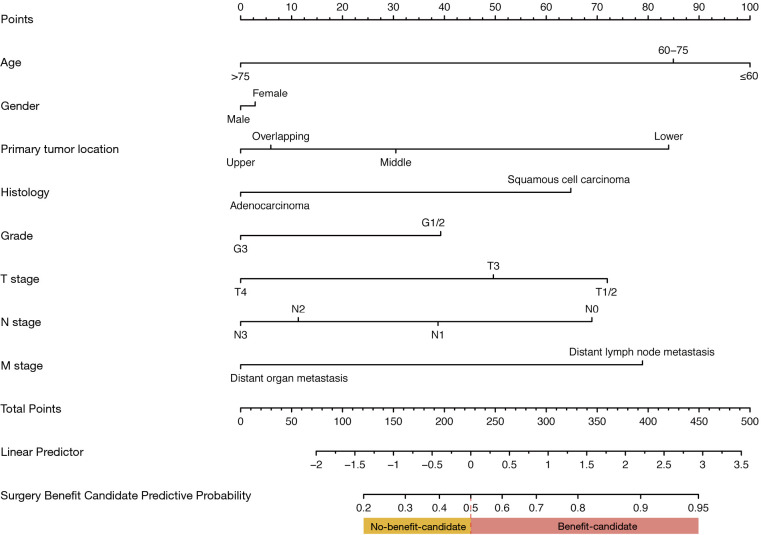
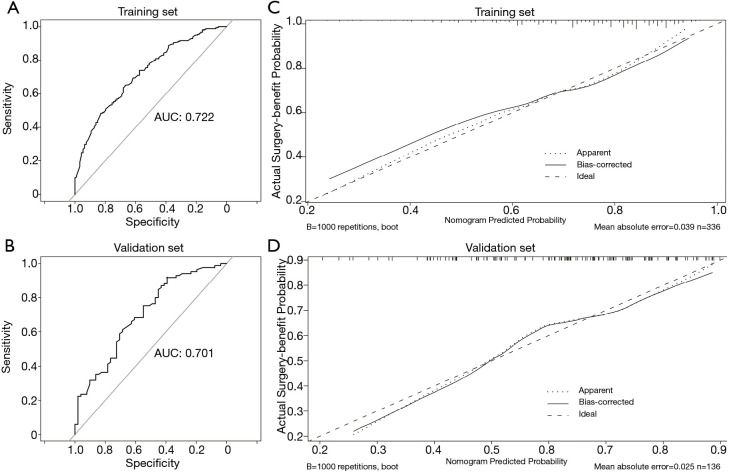
Clinical data for patients with mEC were extracted from the Surveillance, Epidemiology and End Results (SEER) database [2004-2016] and then divided into surgery and no-surgery groups according to whether surgery was performed on the primary tumor. Propensity-score-matching (PSM) was performed to balance the confounding factors. We hypothesized that the patients who had undergone surgery and lived longer than the median cancer-specific-survival (CSS) of the no-surgery group could benefit from surgery. We constructed a nomogram to predict surgery benefit potential based on multivariable logistic-regression analysis using preoperative factors. The predictive performance of the nomogram was evaluated by the area under the receiver operating characteristic (AUC) and calibration curves. The clinical application value of the nomogram was estimated with decision curve analysis (DCA).
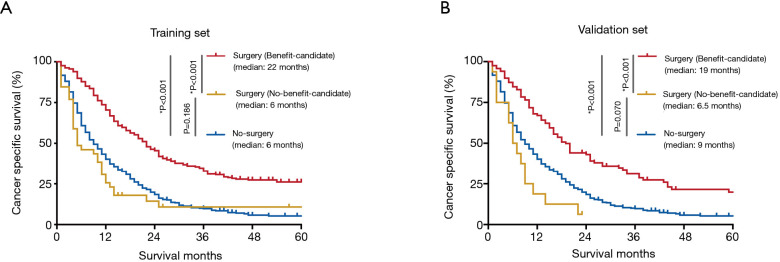
A total of 5,250 eligible patients with mEC were identified, and 9.4% [492] received primary tumor surgery. After PSM, CSS for the surgery group was significantly longer [median: 19 9 months; hazard ratio (HR) 0.52, P<0.001] compared with the no-surgery group. Among the surgery group, 69.3% [327] survived >9 months (surgery-beneficial group). The prediction nomogram showed good discrimination both in training and validation sets (AUC: 0.72 and 0.70, respectively), and the calibration curves indicated a good consistency. DCA demonstrated that the nomogram was clinically useful. According to this nomogram, surgery patients were classified into two groups: no-benefit-candidate and benefit-candidate. The benefit-candidate group was associated with longer survival than the no-benefit-candidate group (median CSS: 19 6.5 months, P<0.001). Additionally, there was no difference in survival between the no-benefit-candidate and no-surgery groups (median CSS: 6.5 9 months, P=0.070).
A predictive model was created for the selection of candidates for surgical treatment among mEC patients. This predictive model might be used to select patients who may benefit from primary tumor surgery.
已观察到原发性肿瘤手术对转移性食管癌(mEC)患者的生存益处,但对于区分哪些个体患者将从手术中获益的方法,目前尚无明确界定。在此,我们开发了一种预测模型,以验证仅某些转移性患者能从原发性肿瘤手术中获得生存益处这一假设。
从监测、流行病学和最终结果(SEER)数据库[2004 - 2016]中提取mEC患者的临床数据,然后根据原发性肿瘤是否接受手术,将患者分为手术组和非手术组。进行倾向得分匹配(PSM)以平衡混杂因素。我们假设接受手术且生存时间超过非手术组癌症特异性生存(CSS)中位数的患者能从手术中获益。我们基于术前因素,通过多变量逻辑回归分析构建了一个列线图,以预测手术获益潜力。通过受试者操作特征曲线(AUC)下面积和校准曲线评估列线图的预测性能。用决策曲线分析(DCA)评估列线图的临床应用价值。
共确定了5250例符合条件的mEC患者,其中9.4%[492例]接受了原发性肿瘤手术。PSM后,手术组的CSS明显长于非手术组[中位数:19.9个月;风险比(HR)0.52,P<0.001]。在手术组中,69.3%[327例]存活超过9个月(手术获益组)。预测列线图在训练集和验证集中均显示出良好的区分度(AUC分别为0.72和0.70),校准曲线显示出良好的一致性。DCA表明列线图具有临床实用性。根据此列线图,手术患者被分为两组:无获益候选组和获益候选组。获益候选组的生存时间长于无获益候选组(CSS中位数:19.6.5个月,P<0.001)。此外,无获益候选组和非手术组的生存情况无差异(CSS中位数:6.5.9个月,P = 0.070)。
创建了一种预测模型,用于在mEC患者中选择手术治疗候选者。该预测模型可能用于选择可能从原发性肿瘤手术中获益的患者。