Pisano Calogera, Farinaccio Andrea, Altieri Claudia, Ajello Valentina, Nardi Paolo, Colella Dionisio Ferdinando, Ruvolo Giovanni
Cardiac Surgery Unit, Department of Surgical Science, Tor Vergata University Hospital, Rome, Italy.
Cardiac and Thoracic Anesthesia Unit, Tor Vergata University Hospital, Rome, Italy.
J Thorac Dis. 2021 Feb;13(2):1011-1019. doi: 10.21037/jtd-20-3032.
Minimally invasive approach through a right mini-thoracotomy is a world-wide used procedure for mitral valve surgery. We performed a retrospective analysis based on our center experience in order to propose an effective, safe and reproducible method using an intra-aortic occlusion device.
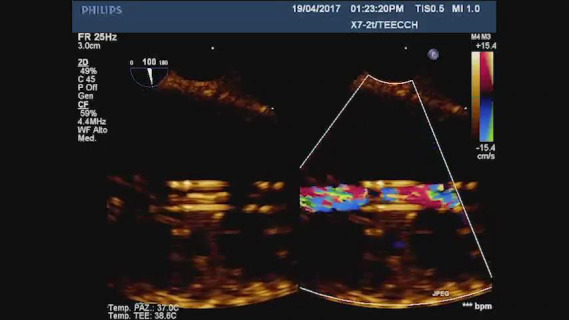
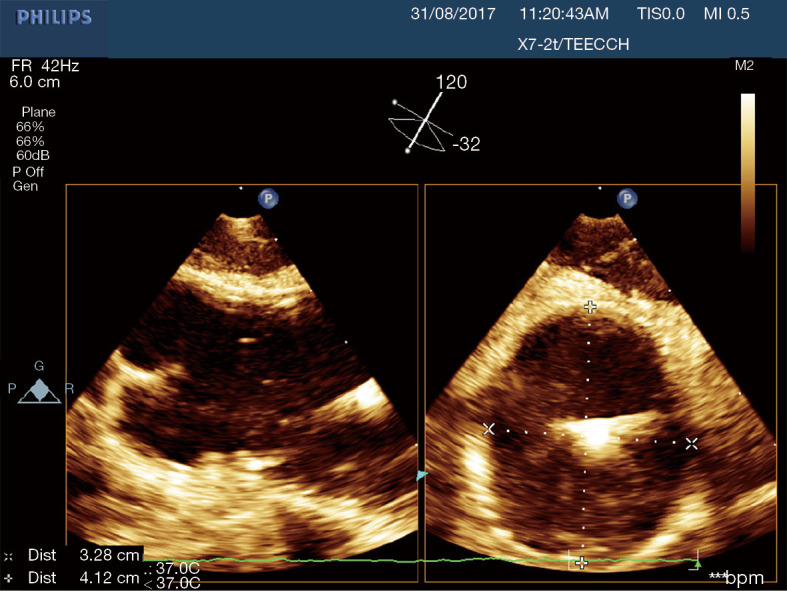
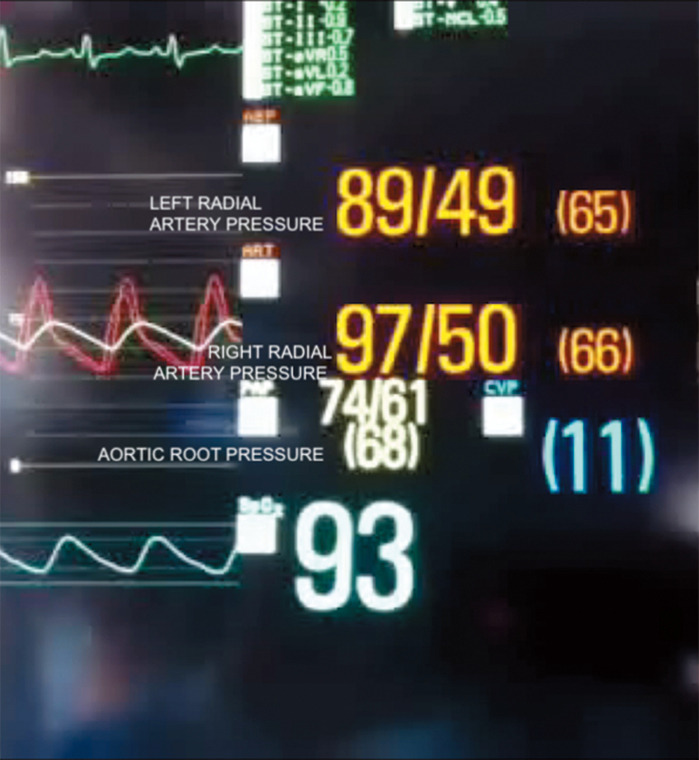
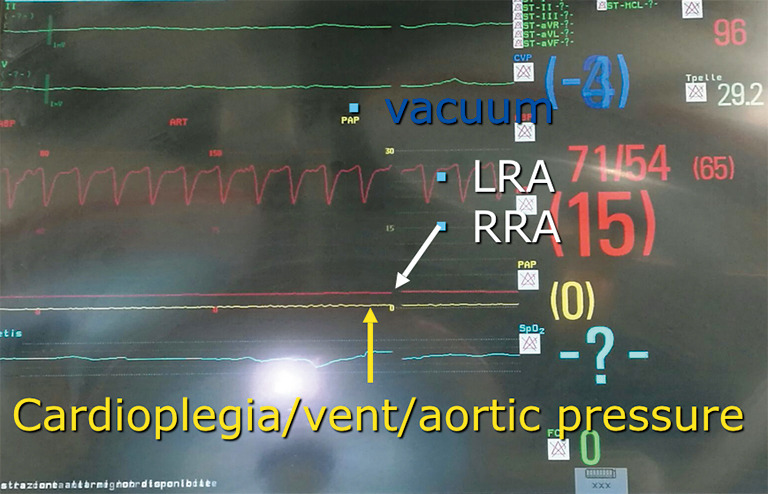
This is a retrospective analysis on 48 consecutive patients undergoing mitral valve surgery through a right anterolateral mini-thoracotomy in our center. An intra-aortic occlusion device was used for aortic clamping and cardioplegia delivery. Simultaneous multi-plane three-dimensional echocardiography imaging was acquired to detect the venous cannulas position, the intra-aortic device location in the ascending aorta, the balloon inflation, the complete occlusion of the aorta, the cardioplegia delivery, the origin and the blood flow in the right coronary artery. Aortic root pressure was measured by the tip of the intra-aortic occlusion device. A bilateral upper extremity invasive arterial pressure monitoring was detected. Neuromonitoring was performed through bilateral cerebral oximetry.
The analysis has shown no aortic dissection, neurological damage type 1 and myocardial ischemia in the study population. In 3 cases a distal displacement of the intra-aortic occlusion device was promptly detected by the combined use of echocardiographic imaging and by a drop of the right cerebral oximetry saturation and of the right radial artery pressure.
The combined use of transesophageal simultaneous multi-plane three- dimensional echocardiography imaging, bilateral upper extremity invasive arterial pressure monitoring, aortic root pressure and cerebral oximetry is an effective, safe and reproducible method in patients undergoing minimally invasive valve surgery using an intra-aortic occlusion device.
经右胸小切口的微创方法是二尖瓣手术在全球范围内广泛应用的术式。我们基于本中心的经验进行了一项回顾性分析,以提出一种使用主动脉内阻断装置的有效、安全且可重复的方法。
这是一项对本中心48例连续接受经右前外侧小切口二尖瓣手术患者的回顾性分析。使用主动脉内阻断装置进行主动脉阻断和心脏停搏液灌注。同时采集多平面三维超声心动图成像,以检测静脉插管位置、主动脉内装置在升主动脉中的位置、球囊充盈情况、主动脉的完全阻断、心脏停搏液灌注、右冠状动脉的起源和血流。通过主动脉内阻断装置的尖端测量主动脉根部压力。进行双侧上肢有创动脉压监测。通过双侧脑氧饱和度监测进行神经监测。
分析显示研究人群中未出现主动脉夹层、1型神经损伤和心肌缺血。在3例患者中,通过超声心动图成像以及右侧脑氧饱和度和右侧桡动脉压力的下降,及时检测到主动脉内阻断装置的远端移位。
对于使用主动脉内阻断装置进行微创瓣膜手术的患者,联合使用经食管同步多平面三维超声心动图成像、双侧上肢有创动脉压监测、主动脉根部压力和脑氧饱和度监测是一种有效、安全且可重复的方法。