Mullins Brandon T, Moore Dominic T, Rivera M Patricia, Marks Lawrence B, Akulian Jason, Pearlstein Kevin A, Wang Kyle, Burks Allen C, Weiner Ashley A
Department of Radiation Oncology, University of North Carolina Hospitals, Chapel Hill, NC, USA.
Lineberger Comprehensive Cancer Center, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA.
J Thorac Dis. 2021 Feb;13(2):1045-1054. doi: 10.21037/jtd-20-2808.
The importance of invasive mediastinal nodal staging in early-stage non-small cell lung cancer (NSCLC) in the PET/CT era is dependent on tumor factors that increase risk of nodal metastasis. At our institution, patients undergo biopsy via either CT-guidance (without nodal staging) or navigational bronchoscopy with endobronchial ultrasound transbronchial needle aspiration for nodal staging. This study aims to compare outcomes after stereotactic body radiotherapy (SBRT) stratified by receipt of invasive mediastinal nodal staging.
In this retrospective study, records of all consecutive patients undergoing SBRT for early-stage NSCLC between 2010 and 2017 were analyzed. The association between time-to event outcomes (recurrence and survival) were evaluated with covariates of interest including tumor size, location, histology, smoking history, prior lung cancer history, radiation dose and receipt of nodal staging. Both univariable and multivariable analyses were used to examine these comparisons.
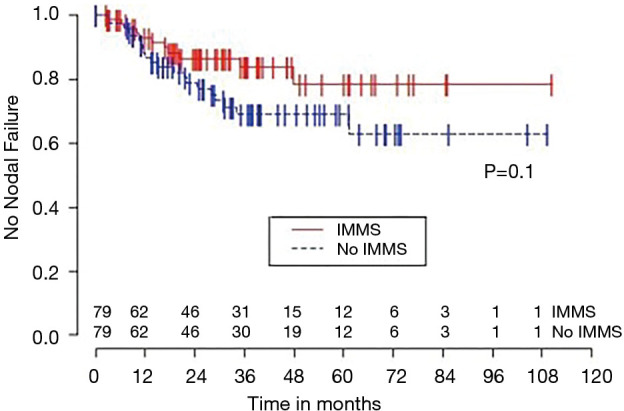
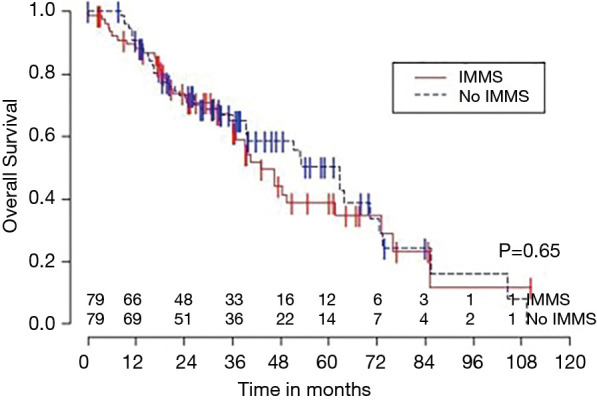
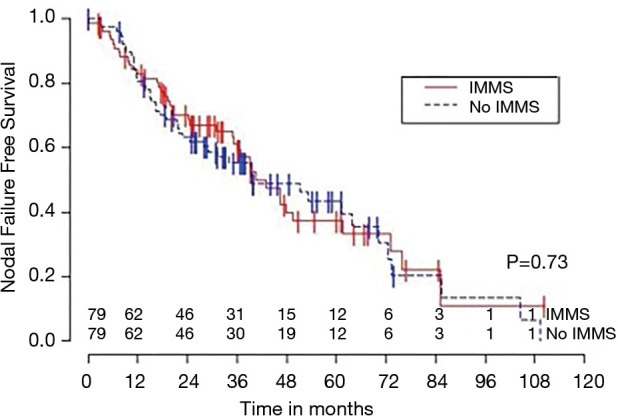
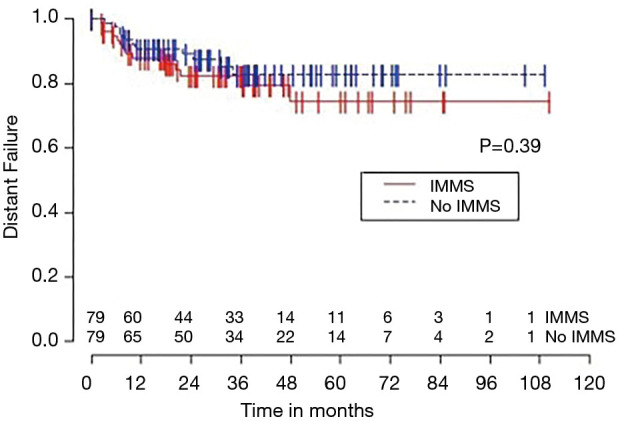
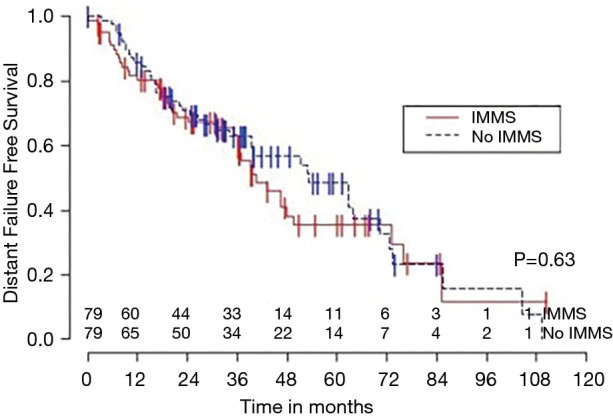
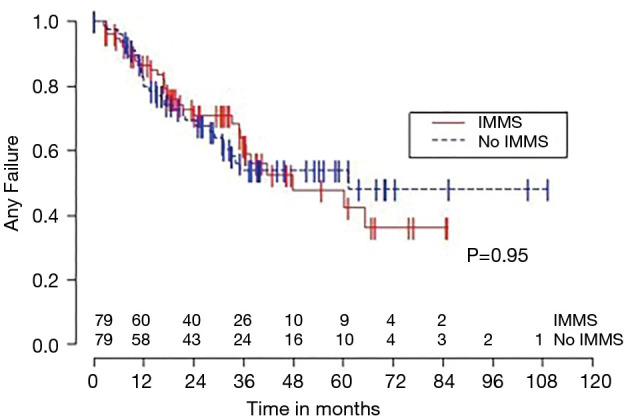
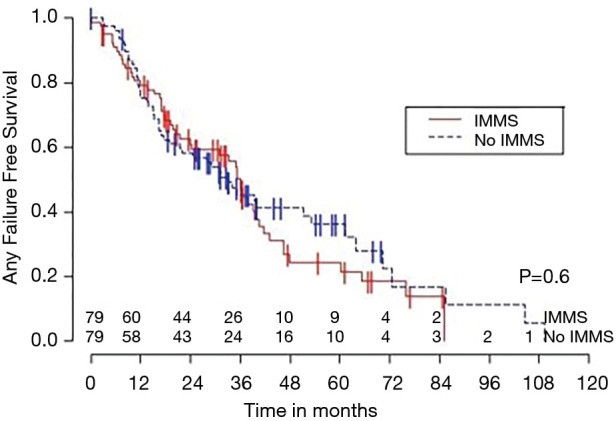
Overall, 158 patients were treated with SBRT. One hundred forty-nine out of one hundred fifty-eight patients (94%) underwent PET/CT staging, and all patients underwent tumor-directed biopsy. Seventy-nine patients underwent navigational bronchoscopy with nodal staging and 79 patients underwent CT-guided biopsy without nodal staging. Receipt of nodal staging was not associated with tumor size (P=0.35), yet was associated with central tumor location (P<0.001). There was no statistically significant association between receipt of nodal staging and time-to-event recurrence or survival outcomes; for example 3-year overall survival (OS) was 65% 67% (P=0.65) and 3-year freedom from nodal failure was 84% 69% (P=0.1) for those with and without nodal staging, respectively.
Similar recurrence and survival outcomes were observed after SBRT regardless of receipt of invasive mediastinal nodal staging. Further prospective evaluation can help identify which patients might derive greatest benefit from invasive staging of the mediastinum in the PET/CT era.
在PET/CT时代,侵袭性纵隔淋巴结分期在早期非小细胞肺癌(NSCLC)中的重要性取决于增加淋巴结转移风险的肿瘤因素。在我们机构,患者通过CT引导活检(无淋巴结分期)或经支气管镜超声引导经支气管针吸活检进行淋巴结分期的导航支气管镜检查。本研究旨在比较接受侵袭性纵隔淋巴结分期分层的立体定向体部放疗(SBRT)后的结果。
在这项回顾性研究中,分析了2010年至2017年间所有连续接受SBRT治疗的早期NSCLC患者的记录。使用包括肿瘤大小、位置、组织学、吸烟史、既往肺癌史、放射剂量和淋巴结分期情况等感兴趣的协变量评估事件发生时间结局(复发和生存)之间的关联。采用单变量和多变量分析来检验这些比较。
总体而言,158例患者接受了SBRT治疗。158例患者中有149例(94%)接受了PET/CT分期,所有患者均接受了肿瘤靶向活检。79例患者接受了有淋巴结分期的导航支气管镜检查,79例患者接受了无淋巴结分期的CT引导活检。接受淋巴结分期与肿瘤大小无关(P=0.35),但与肿瘤中央位置有关(P<0.001)。接受淋巴结分期与事件发生时间复发或生存结局之间无统计学显著关联;例如,有和无淋巴结分期的患者3年总生存率(OS)分别为65%和67%(P=0.65),3年无淋巴结转移生存率分别为84%和69%(P=0.1)。
无论是否接受侵袭性纵隔淋巴结分期。在SBRT后观察到相似的复发和生存结果。进一步的前瞻性评估有助于确定在PET/CT时代哪些患者可能从纵隔侵袭性分期中获益最大。