Rodríguez María, Ajona Daniel, Seijo Luis M, Sanz Julián, Valencia Karmele, Corral Jesús, Mesa-Guzmán Miguel, Pío Rubén, Calvo Alfonso, Lozano María D, Zulueta Javier J, Montuenga Luis M
Department of Thoracic Surgery, Clínica Universidad de Navarra, Madrid, Spain.
Program in Solid Tumors, Center for Applied Medical Research (CIMA), University of Navarra, Pamplona, Spain.
Transl Lung Cancer Res. 2021 Feb;10(2):1165-1185. doi: 10.21037/tlcr-20-750.
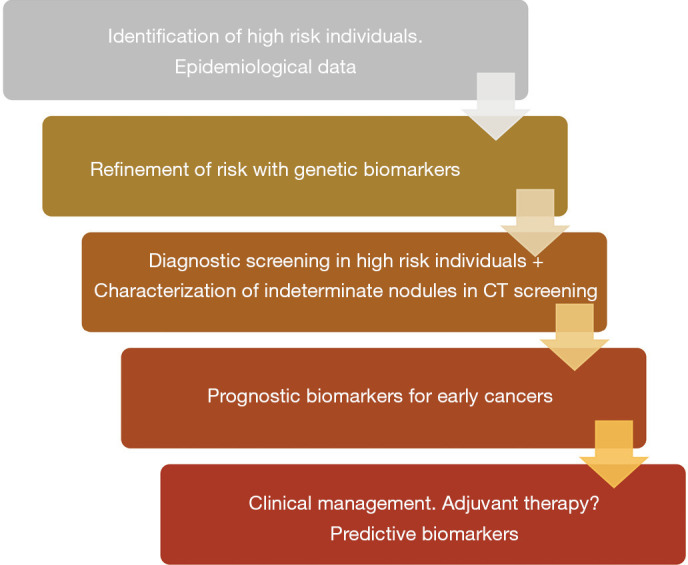
Low dose computed tomography (LDCT) screening, together with the recent advances in targeted and immunotherapies, have shown to improve non-small cell lung cancer (NSCLC) survival. Furthermore, screening has increased the number of early stage-detected tumors, allowing for surgical resection and multimodality treatments when needed. The need for improved sensitivity and specificity of NSCLC screening has led to increased interest in combining clinical and radiological data with molecular data. The development of biomarkers is poised to refine inclusion criteria for LDCT screening programs. Biomarkers may also be useful to better characterize the risk of indeterminate nodules found in the course of screening or to refine prognosis and help in the management of screening detected tumors. The clinical implications of these biomarkers are still being investigated and whether or not biomarkers will be included in further decision-making algorithms in the context of screening and early lung cancer management still needs to be determined. However, it seems clear that there is much room for improvement even in early stage lung cancer disease-free survival (DFS) rates; thus, biomarkers may be the key to refine risk-stratification and treatment of these patients. Clinicians' capacity to register, integrate, and analyze all the available data in both high risk individuals and early stage NSCLC patients will lead to a better understanding of the disease's mechanisms, and will have a direct impact in diagnosis, treatment, and follow up of these patients. In this review, we aim to summarize all the available data regarding the role of biomarkers in LDCT screening and early stage NSCLC from a multidisciplinary perspective. We have highlighted clinical implications, the need to combine risk stratification, clinical data, radiomics, molecular information and artificial intelligence in order to improve clinical decision-making, especially regarding early diagnostics and adjuvant therapy. We also discuss current and future perspectives for biomarker implementation in routine clinical practice.
低剂量计算机断层扫描(LDCT)筛查,连同靶向治疗和免疫治疗的最新进展,已显示可提高非小细胞肺癌(NSCLC)患者的生存率。此外,筛查增加了早期发现肿瘤的数量,使得在需要时能够进行手术切除和多模式治疗。对提高NSCLC筛查的敏感性和特异性的需求,引发了将临床和放射学数据与分子数据相结合的兴趣增加。生物标志物的发展有望完善LDCT筛查项目的纳入标准。生物标志物也可能有助于更好地描述筛查过程中发现的不确定结节的风险,或完善预后评估,并有助于管理筛查发现的肿瘤。这些生物标志物的临床意义仍在研究中,在筛查和早期肺癌管理的背景下,生物标志物是否会被纳入进一步的决策算法仍有待确定。然而,很明显,即使在早期肺癌无病生存率(DFS)方面仍有很大的改善空间;因此,生物标志物可能是优化这些患者风险分层和治疗的关键。临床医生对高危个体和早期NSCLC患者所有可用数据进行记录、整合和分析的能力,将有助于更好地理解疾病机制,并将直接影响这些患者的诊断、治疗和随访。在本综述中,我们旨在从多学科角度总结关于生物标志物在LDCT筛查和早期NSCLC中的作用的所有可用数据。我们强调了临床意义,以及为改善临床决策,特别是关于早期诊断和辅助治疗,将风险分层、临床数据、放射组学、分子信息和人工智能相结合的必要性。我们还讨论了生物标志物在常规临床实践中应用的当前和未来前景。