Nasa Prashant, Azoulay Elie, Khanna Ashish K, Jain Ravi, Gupta Sachin, Javeri Yash, Juneja Deven, Rangappa Pradeep, Sundararajan Krishnaswamy, Alhazzani Waleed, Antonelli Massimo, Arabi Yaseen M, Bakker Jan, Brochard Laurent J, Deane Adam M, Du Bin, Einav Sharon, Esteban Andrés, Gajic Ognjen, Galvagno Samuel M, Guérin Claude, Jaber Samir, Khilnani Gopi C, Koh Younsuck, Lascarrou Jean-Baptiste, Machado Flavia R, Malbrain Manu L N G, Mancebo Jordi, McCurdy Michael T, McGrath Brendan A, Mehta Sangeeta, Mekontso-Dessap Armand, Mer Mervyn, Nurok Michael, Park Pauline K, Pelosi Paolo, Peter John V, Phua Jason, Pilcher David V, Piquilloud Lise, Schellongowski Peter, Schultz Marcus J, Shankar-Hari Manu, Singh Suveer, Sorbello Massimiliano, Tiruvoipati Ravindranath, Udy Andrew A, Welte Tobias, Myatra Sheila N
Critical Care Medicine, NMC Speciality Hospital, Dubai, United Arab Emirates.
Saint-Louis teaching hospital - APHP - and University of Paris, Paris, France.
Crit Care. 2021 Mar 16;25(1):106. doi: 10.1186/s13054-021-03491-y.
Coronavirus disease 2019 (COVID-19) pandemic has caused unprecedented pressure on healthcare system globally. Lack of high-quality evidence on the respiratory management of COVID-19-related acute respiratory failure (C-ARF) has resulted in wide variation in clinical practice.
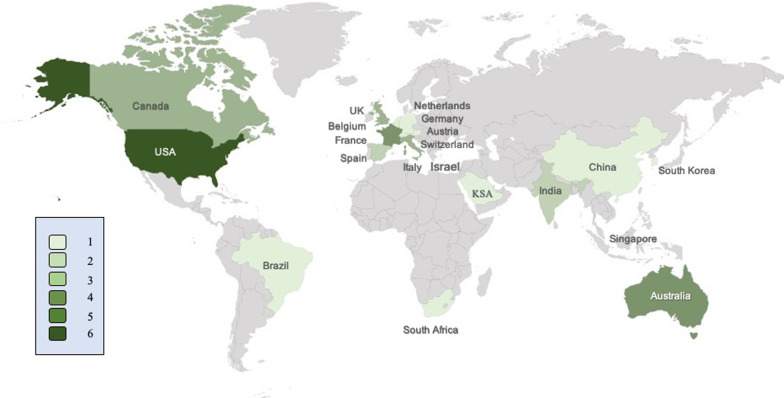
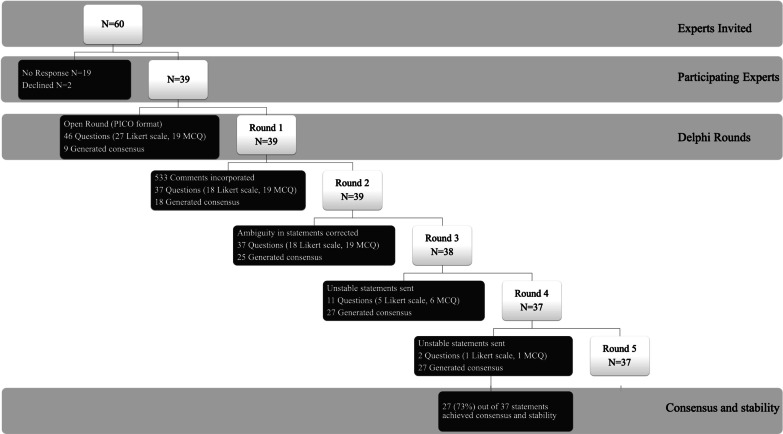
Using a Delphi process, an international panel of 39 experts developed clinical practice statements on the respiratory management of C-ARF in areas where evidence is absent or limited. Agreement was defined as achieved when > 70% experts voted for a given option on the Likert scale statement or > 80% voted for a particular option in multiple-choice questions. Stability was assessed between the two concluding rounds for each statement, using the non-parametric Chi-square (χ) test (p < 0·05 was considered as unstable).
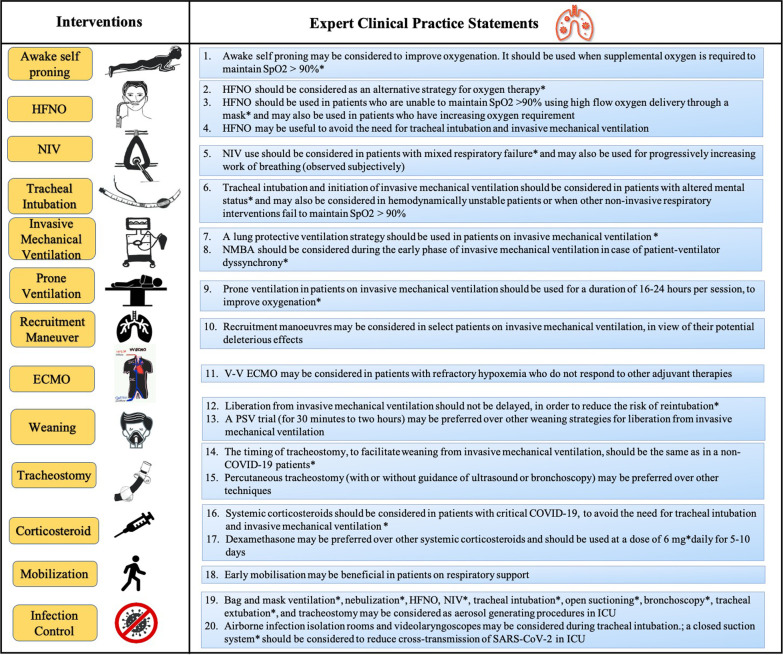
Agreement was achieved for 27 (73%) management strategies which were then used to develop expert clinical practice statements. Experts agreed that COVID-19-related acute respiratory distress syndrome (ARDS) is clinically similar to other forms of ARDS. The Delphi process yielded strong suggestions for use of systemic corticosteroids for critical COVID-19; awake self-proning to improve oxygenation and high flow nasal oxygen to potentially reduce tracheal intubation; non-invasive ventilation for patients with mixed hypoxemic-hypercapnic respiratory failure; tracheal intubation for poor mentation, hemodynamic instability or severe hypoxemia; closed suction systems; lung protective ventilation; prone ventilation (for 16-24 h per day) to improve oxygenation; neuromuscular blocking agents for patient-ventilator dyssynchrony; avoiding delay in extubation for the risk of reintubation; and similar timing of tracheostomy as in non-COVID-19 patients. There was no agreement on positive end expiratory pressure titration or the choice of personal protective equipment.
Using a Delphi method, an agreement among experts was reached for 27 statements from which 20 expert clinical practice statements were derived on the respiratory management of C-ARF, addressing important decisions for patient management in areas where evidence is either absent or limited.
The study was registered with Clinical trials.gov Identifier: NCT04534569.
2019年冠状病毒病(COVID-19)大流行给全球医疗系统带来了前所未有的压力。缺乏关于COVID-19相关急性呼吸衰竭(C-ARF)呼吸管理的高质量证据,导致临床实践差异很大。
通过德尔菲法,一个由39名专家组成的国际小组针对证据缺乏或有限的领域,制定了关于C-ARF呼吸管理的临床实践声明。当超过70%的专家在李克特量表声明中对某个选项投赞成票,或在多项选择题中超过80%的专家对某个特定选项投赞成票时,即达成共识。使用非参数卡方(χ)检验评估每个声明在两轮总结之间的稳定性(p<0.05被认为不稳定)。
27项(73%)管理策略达成了共识,随后用于制定专家临床实践声明。专家们一致认为,COVID-19相关急性呼吸窘迫综合征(ARDS)在临床上与其他形式的ARDS相似。德尔菲法产生了关于以下方面的强烈建议:对重症COVID-19患者使用全身皮质类固醇;清醒自主俯卧位以改善氧合,高流量鼻导管吸氧以潜在减少气管插管;对低氧血症合并高碳酸血症呼吸衰竭患者进行无创通气;对意识障碍、血流动力学不稳定或严重低氧血症患者进行气管插管;使用密闭式吸痰系统;采用肺保护性通气;俯卧位通气(每天16 - 24小时)以改善氧合;对患者-呼吸机不同步使用神经肌肉阻滞剂;避免因再插管风险而延迟拔管;以及气管切开时机与非COVID-19患者相似。在呼气末正压滴定或个人防护设备的选择上未达成共识。
采用德尔菲法,专家们就27项声明达成了共识,从中得出了20项关于C-ARF呼吸管理的专家临床实践声明,解决了证据缺乏或有限领域中患者管理的重要决策问题。
该研究已在Clinicaltrials.gov注册,标识符:NCT04534569。