Clinical Pharmacology and Quantitative Pharmacology, Clinical Pharmacology and Safety Sciences, R&D, AstraZeneca, Gothenburg, Sweden.
Clinical Pharmacology and Quantitative Pharmacology, Clinical Pharmacology and Safety Sciences, R&D, AstraZeneca, Waltham, MA, USA.
J Pharmacokinet Pharmacodyn. 2021 Aug;48(4):525-541. doi: 10.1007/s10928-021-09747-y. Epub 2021 Mar 17.
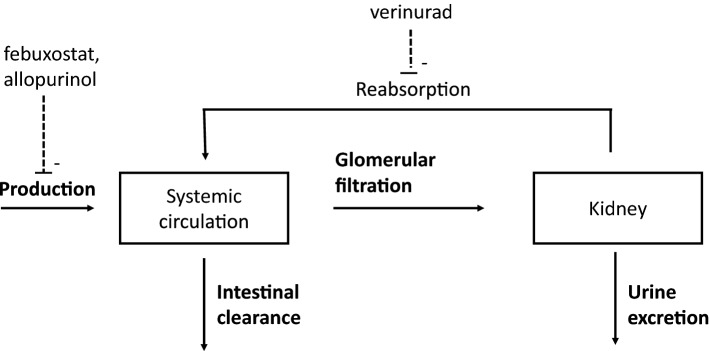
Verinurad, a uric acid transporter 1 (URAT1) inhibitor, lowers serum uric acid by promoting its urinary excretion. Co-administration with a xanthine oxidase inhibitor (XOI) to simultaneously reduce uric acid production rate reduces the potential for renal tubular precipitation of uric acid, which can lead to acute kidney injury. The combination is currently in development for chronic kidney disease and heart failure. The aim of this work was to apply and extend a previously developed semi-mechanistic exposure-response model for uric acid kinetics to include between-subject variability to verinurad and its combinations with XOIs, and to provide predictions to support future treatment strategies. The model was developed using data from 12 clinical studies from a total of 434 individuals, including healthy volunteers, patients with hyperuricemia, and renally impaired subjects. The model described the data well, taking into account the impact of various patient characteristics such as renal function, baseline fractional excretion of uric acid, and race. The potencies (EC50s) of verinurad (reducing uric acid reuptake), febuxostat (reducing uric acid production), and oxypurinol (reducing uric acid production) were: 29, 128, and 13,030 ng/mL, respectively. For verinurad, symptomatic hyperuricemic (gout) subjects showed a higher EC50 compared with healthy volunteers (37 ng/mL versus 29 ng/mL); while no significant difference was found for asymptomatic hyperuricemic patients. Simulations based on the uric acid model were performed to assess dose-response of verinurad in combination with XOI, and to investigate the impact of covariates. The simulations demonstrated application of the model to support dose selection for verinurad.
维那鲁单抗是一种尿酸转运蛋白 1(URAT1)抑制剂,通过促进其尿液排泄来降低血清尿酸水平。与黄嘌呤氧化酶抑制剂(XOI)联合使用,同时降低尿酸生成率,降低尿酸在肾小管中沉淀的潜力,从而导致急性肾损伤。该联合用药目前正在开发用于慢性肾病和心力衰竭。本研究旨在应用和扩展先前开发的尿酸动力学半机制暴露-反应模型,将其扩展到包括维那鲁单抗及其与 XOI 组合的个体间变异性,并提供预测结果以支持未来的治疗策略。该模型是使用来自总共 434 名个体的 12 项临床研究的数据开发的,包括健康志愿者、高尿酸血症患者和肾功能受损患者。该模型很好地描述了数据,考虑了各种患者特征的影响,如肾功能、尿酸的基础分数排泄率和种族。维那鲁单抗(减少尿酸重吸收)、非布司他(减少尿酸生成)和奥昔嘌醇(减少尿酸生成)的效价(EC50)分别为 29、128 和 13030ng/mL。对于维那鲁单抗,有症状的高尿酸血症(痛风)患者与健康志愿者相比,其 EC50 更高(37ng/mL 比 29ng/mL);而无症状高尿酸血症患者则没有发现显著差异。基于尿酸模型的模拟用于评估维那鲁单抗与 XOI 联合用药的剂量反应,并研究协变量的影响。模拟结果表明,可以将该模型应用于支持维那鲁单抗的剂量选择。