Centers for Disease Control and Prevention, COVID-19 Response, 4770 Buford Highway, Atlanta, GA, 30341, USA.
Global Health. 2021 Mar 17;17(1):28. doi: 10.1186/s12992-021-00678-4.
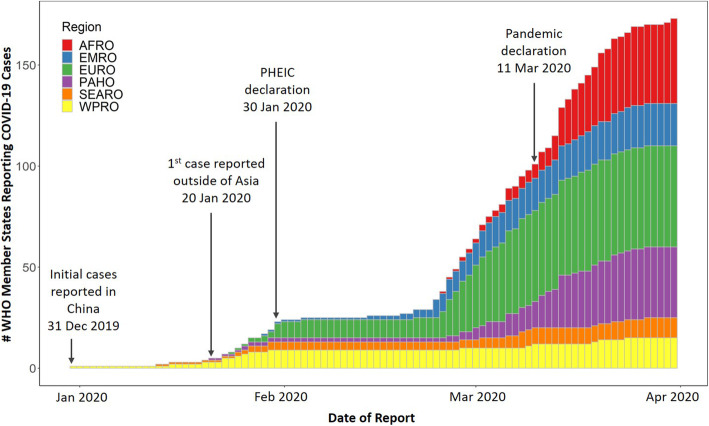
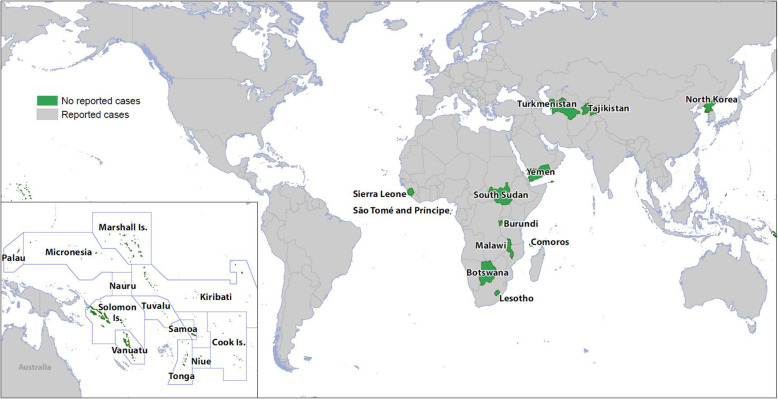
Three months after the first reported cases, COVID-19 had spread to nearly 90% of World Health Organization (WHO) member states and only 24 countries had not reported cases as of 30 March 2020. This analysis aimed to 1) assess characteristics, capability to detect and monitor COVID-19, and disease control measures in these 24 countries, 2) understand potential factors for the reported delayed COVID-19 introduction, and 3) identify gaps and opportunities for outbreak preparedness, particularly in low and middle-income countries (LMICs). We collected and analyzed publicly available information on country characteristics, COVID-19 testing, influenza surveillance, border measures, and preparedness activities in these countries. We also assessed the association between the temporal spread of COVID-19 in all countries with reported cases with globalization indicator and geographic location.
Temporal spreading of COVID-19 was strongly associated with countries' globalization indicator and geographic location. Most of the 24 countries with delayed COVID-19 introduction were LMICs; 88% were small island or landlocked developing countries. As of 30 March 2020, only 38% of these countries reported in-country COVID-19 testing capability, and 71% reported conducting influenza surveillance during the past year. All had implemented two or more border measures, (e.g., travel restrictions and border closures) and multiple preparedness activities (e.g., national preparedness plans and school closing).
Limited testing capacity suggests that most of the 24 delayed countries may have lacked the capability to detect and identify cases early through sentinel and case-based surveillance. Low global connectedness, geographic isolation, and border measures were common among these countries and may have contributed to the delayed introduction of COVID-19 into these countries. This paper contributes to identifying opportunities for pandemic preparedness, such as increasing disease detection, surveillance, and international collaborations. As the global situation continues to evolve, it is essential for countries to improve and prioritize their capacities to rapidly prevent, detect, and respond, not only for COVID-19, but also for future outbreaks.
自首例报告病例以来的三个月内,COVID-19 已传播至世界卫生组织(WHO)几乎 90%的成员国,截至 2020 年 3 月 30 日,仅有 24 个国家尚未报告病例。本分析旨在:1)评估这 24 个国家的 COVID-19 的特征、检测和监测能力以及疾病控制措施;2)了解报告 COVID-19 延迟引入的潜在因素;3)确定暴发准备工作中的差距和机会,特别是在中低收入国家(LMICs)。我们收集并分析了这些国家在国家特征、COVID-19 检测、流感监测、边境措施和备灾活动方面的公开信息。我们还评估了所有报告病例的国家中 COVID-19 的时间传播与全球化指标和地理位置之间的关联。
COVID-19 的时间传播与国家的全球化指标和地理位置密切相关。报告 COVID-19 延迟引入的 24 个国家中,大多数是中低收入国家;88%是小岛或内陆发展中国家。截至 2020 年 3 月 30 日,这些国家中只有 38%报告了国内 COVID-19 检测能力,71%报告了过去一年的流感监测。所有国家都实施了两项或更多项边境措施(如旅行限制和边境关闭)和多项备灾活动(如国家备灾计划和学校关闭)。
检测能力有限表明,大部分延迟国家可能缺乏通过哨点和基于病例的监测及早发现和识别病例的能力。这些国家普遍存在低全球连通性、地理位置孤立和边境措施,这可能导致 COVID-19 延迟传入这些国家。本文有助于确定大流行准备工作的机会,例如增加疾病检测、监测和国际合作。随着全球形势的不断发展,各国必须提高和优先考虑快速预防、检测和应对的能力,不仅针对 COVID-19,还针对未来的疫情暴发。