Metro South Integrated Nephrology and Transplant Services, Logan Hospital, Armstrong Road & Loganlea Road, Meadowbrook, Queensland, 4131, Australia.
Faculty of Medicine, University of Queensland, Armstrong Road & Loganlea Road, St Lucia, Queensland, 4072, Australia.
BMC Nephrol. 2021 Mar 18;22(1):97. doi: 10.1186/s12882-021-02279-0.
Patients on chronic dialysis are at increased risk of postoperative mortality following elective surgery compared to patients with normal kidney function, but morbidity outcomes are less often reported. This study ascertains the excess odds of postoperative cardiovascular and infection related morbidity outcomes for patients on chronic dialysis.
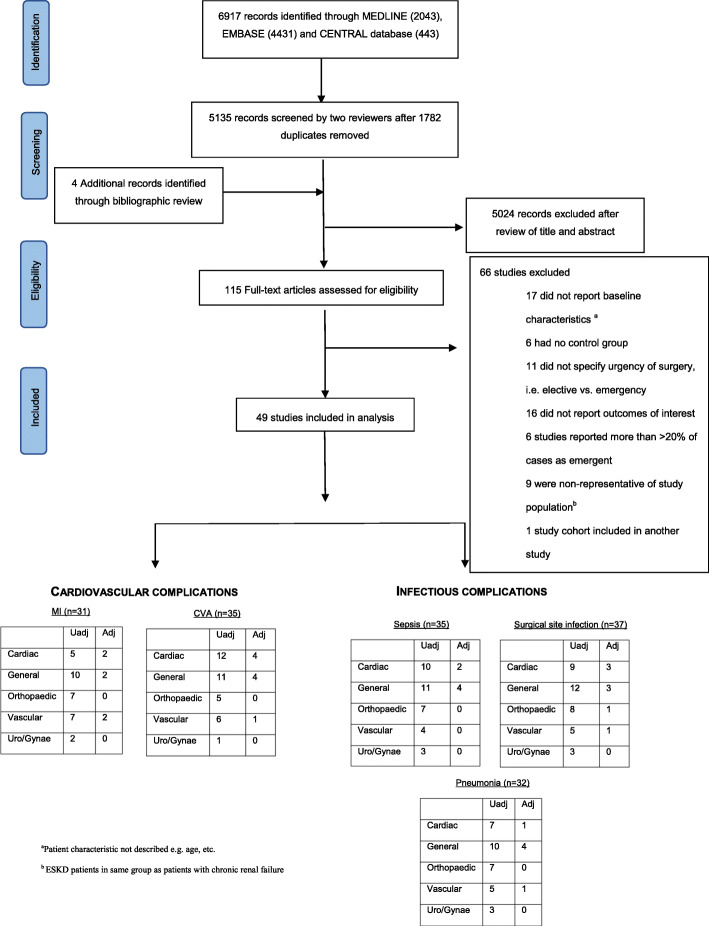
Systematic searches were performed using MEDLINE, Embase and the Cochrane Library to identify relevant studies published from inception to January 2020. Eligible studies reported postoperative morbidity outcomes in chronic dialysis and non-dialysis patients undergoing major non-transplant surgery. Risk of bias was assessed using the Newcastle-Ottawa Scale and the certainty of evidence was summarised using GRADE. Random effects meta-analyses were performed to derive summary odds estimates. Meta-regression and sensitivity analyses were performed to explore heterogeneity.
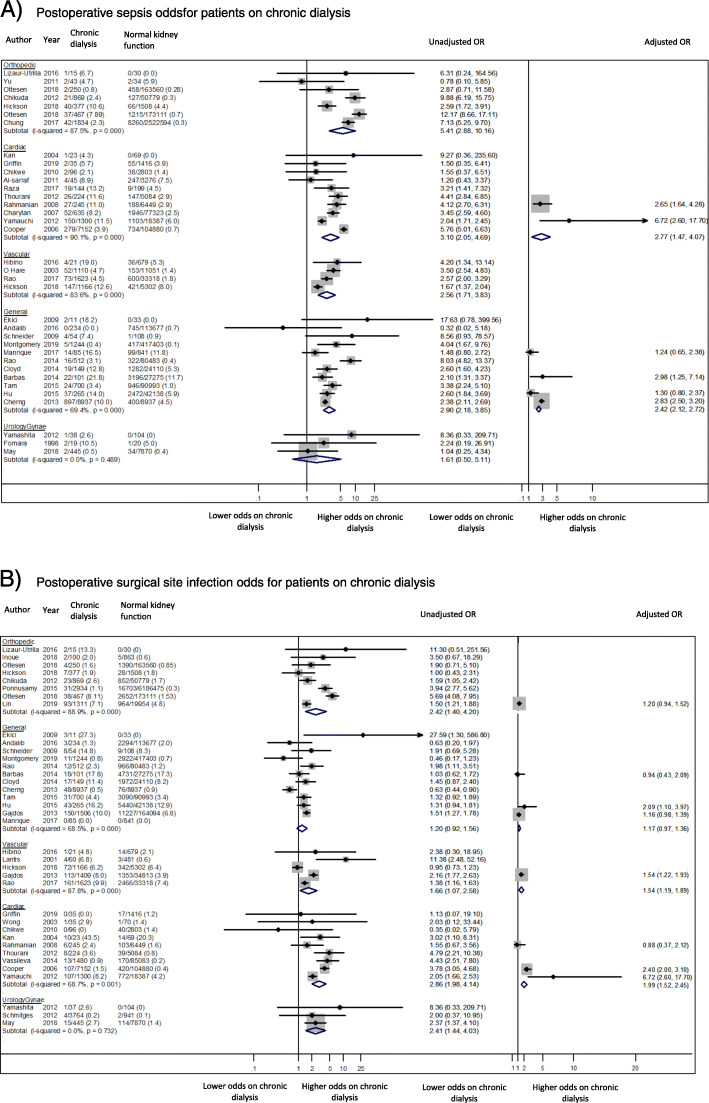
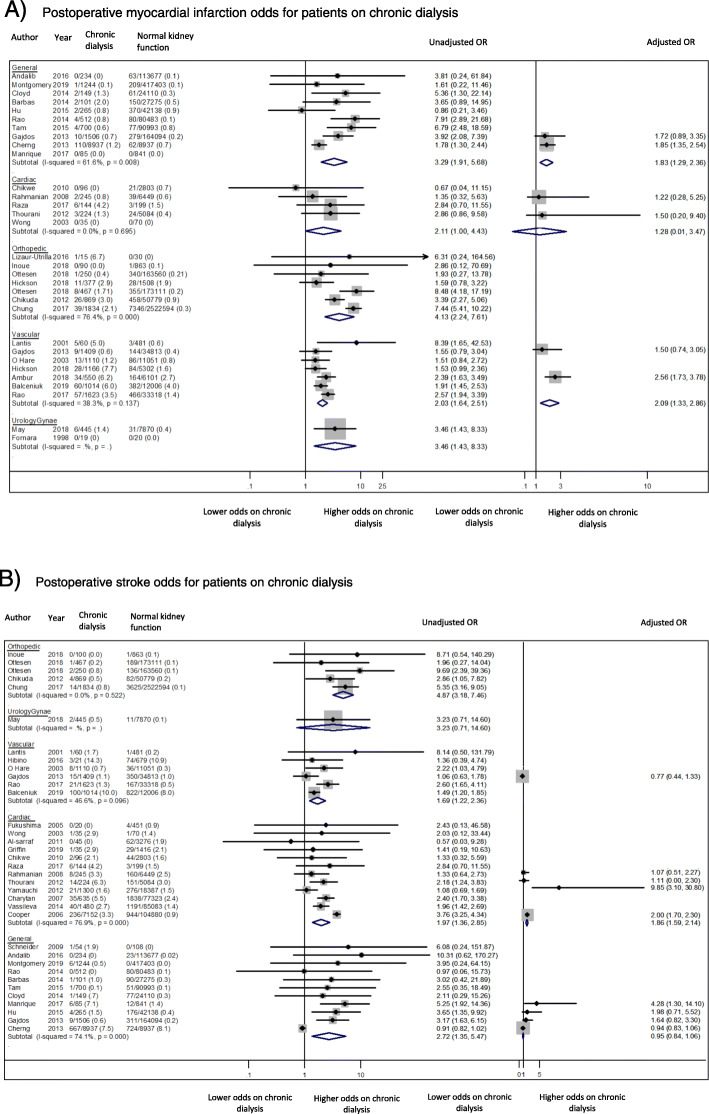
Forty-nine studies involving 10,513,934 patients with normal kidney function and 43,092 patients receiving chronic dialysis were included. Patients on chronic dialysis had increased unadjusted odds of postoperative cardiovascular and infectious complications within each surgical discipline. However, the excess odds of cardiovascular complications was attenuated when odds ratios were adjusted for age and comorbidities; myocardial infarction (general surgery, OR 1.83 95% 1.29-2.36) and stroke (general surgery, OR 0.95, 95%CI 0.84-1.06). The excess odds of infectious complications remained substantially higher for patients on chronic dialysis, particularly sepsis (general surgery, OR 2.42, 95%CI 2.12-2.72).
Patients on chronic dialysis are at increased odds of both cardiovascular and infectious complications following elective surgery, with the excess odds of cardiovascular complications attributable to being on dialysis being highest among younger patients without comorbidities. However, further research is needed to better inform perioperative risk assessment.
与肾功能正常的患者相比,接受择期手术的慢性透析患者术后死亡风险增加,但发病率结果报告较少。本研究确定了慢性透析患者术后心血管和感染相关发病率结果的超额几率。
系统检索 MEDLINE、Embase 和 Cochrane 图书馆,以确定从成立到 2020 年 1 月发表的相关研究。符合条件的研究报告了接受主要非移植手术的慢性透析和非透析患者的术后发病率结果。使用纽卡斯尔-渥太华量表评估偏倚风险,并使用 GRADE 总结证据确定性。进行随机效应荟萃分析以得出汇总优势估计。进行荟萃回归和敏感性分析以探索异质性。
纳入了 49 项研究,涉及 10513934 名肾功能正常患者和 43092 名接受慢性透析的患者。慢性透析患者在每个外科科室中都有增加的未经调整的术后心血管和感染并发症的优势比。然而,当调整了年龄和合并症的比值比时,心血管并发症的超额优势比有所减弱;心肌梗死(普通外科,OR 1.83,95%CI 1.29-2.36)和中风(普通外科,OR 0.95,95%CI 0.84-1.06)。慢性透析患者感染并发症的超额优势仍然明显更高,特别是败血症(普通外科,OR 2.42,95%CI 2.12-2.72)。
接受择期手术的慢性透析患者发生心血管和感染并发症的几率均增加,与透析相关的心血管并发症的超额几率在无合并症的年轻患者中最高。但是,需要进一步研究以更好地告知围手术期风险评估。