Department of Medical Informatics and Clinical Epidemiology, Oregon Health and Science University, 3030 SW Moody Ave, Portland, OR, 97201, USA.
VA Portland Health Care System, Portland, OR, USA.
BMC Med Inform Decis Mak. 2021 Mar 18;21(1):104. doi: 10.1186/s12911-021-01455-4.
Patients with complex health care needs may suffer adverse outcomes from fragmented and delayed care, reducing well-being and increasing health care costs. Health reform efforts, especially those in primary care, attempt to mitigate risk of adverse outcomes by better targeting resources to those most in need. However, predicting who is susceptible to adverse outcomes, such as unplanned hospitalizations, ED visits, or other potentially avoidable expenditures, can be difficult, and providing intensive levels of resources to all patients is neither wanted nor efficient. Our objective was to understand if primary care teams can predict patient risk better than standard risk scores.
Six primary care practices risk stratified their entire patient population over a 2-year period, and worked to mitigate risk for those at high risk through care management and coordination. Individual patient risk scores created by the practices were collected and compared to a common risk score (Hierarchical Condition Categories) in their ability to predict future expenditures, ED visits, and hospitalizations. Accuracy of predictions, sensitivity, positive predictive values (PPV), and c-statistics were calculated for each risk scoring type. Analyses were stratified by whether the practice used intuition alone, an algorithm alone, or adjudicated an algorithmic risk score.
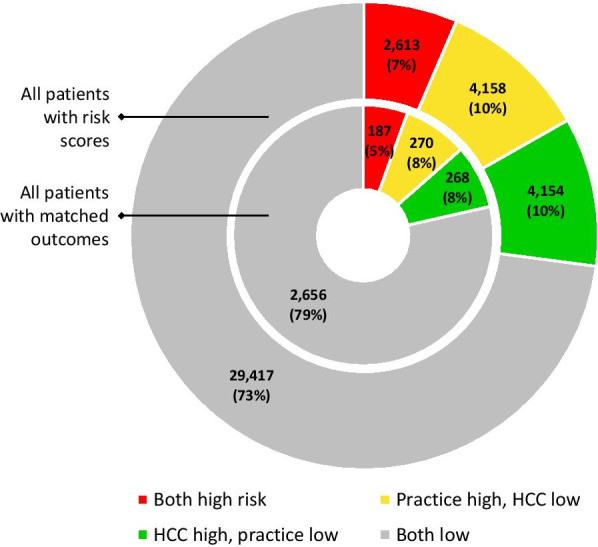
In all, 40,342 patients were risk stratified. Practice scores had 38.6% agreement with HCC scores on identification of high-risk patients. For the 3,381 patients with reliable outcomes data, accuracy was high (0.71-0.88) but sensitivity and PPV were low (0.16-0.40). Practice-created scores had 0.02-0.14 lower sensitivity, specificity and PPV compared to HCC in prediction of outcomes. Practices using adjudication had, on average, .16 higher sensitivity.
Practices using simple risk stratification techniques had slightly worse accuracy in predicting common outcomes than HCC, but adjudication improved prediction.
患有复杂医疗需求的患者可能因医疗服务碎片化和延迟而导致不良后果,降低生活质量并增加医疗成本。医疗改革努力,特别是在初级保健方面,试图通过更好地将资源瞄准最需要的人群来降低不良后果的风险。然而,预测哪些患者容易出现不良后果(如非计划性住院、急诊就诊或其他可能避免的支出)可能具有挑战性,而且向所有患者提供密集的资源既不受欢迎也不高效。我们的目标是了解初级保健团队是否能够比标准风险评分更好地预测患者的风险。
六家初级保健机构在两年内对其所有患者进行风险分层,并通过护理管理和协调来降低高危患者的风险。收集每家机构创建的患者个体风险评分,并将其与常见风险评分(层次条件类别)进行比较,以评估其预测未来支出、急诊就诊和住院的能力。为每种风险评分类型计算预测的准确性、敏感性、阳性预测值(PPV)和 c 统计量。分析按以下分层:机构是否仅使用直觉、仅使用算法,还是使用算法调整后的风险评分。
总共有 40342 名患者进行了风险分层。机构评分与 HCC 评分在识别高危患者方面的一致性为 38.6%。对于有可靠结果数据的 3381 名患者,准确性较高(0.71-0.88),但敏感性和 PPV 较低(0.16-0.40)。与 HCC 相比,机构评分在预测结果方面的敏感性、特异性和 PPV 低 0.02-0.14。使用裁决的机构评分平均具有 0.16 更高的敏感性。
使用简单风险分层技术的机构在预测常见结果方面的准确性略低于 HCC,但裁决可提高预测准确性。