Department of Urology, Icahn School of Medicine at Mount Sinai, New York, New York.
Intuitive Surgical Inc, Sunnyvale, California.
JAMA Netw Open. 2021 Mar 1;4(3):e212265. doi: 10.1001/jamanetworkopen.2021.2265.
With the current patterns of adoption and use of robotic surgery and improvement in the overall survival of patients with prostate cancer, it is important to evaluate the immediate and long-term cost implications of treatments for patients with prostate cancer.
To compare health care costs and use 1 year after open radical prostatectomy (ORP) vs robotic-assisted radical prostatectomy (RARP).
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study used a US commercial claims database from January 1, 2013, to December 31, 2018. A total of 11 457 men aged 18 to 64 years who underwent inpatient radical prostatectomy for prostate cancer and were continuously enrolled with medical and prescription drug coverage from 180 days before to 365 days after inpatient prostatectomy were identified. An inverse probability of treatment weighting analysis was performed to examine the differences in costs and use of health care services by surgical modality. Data analysis was conducted from September 2019 to July 2020.
Type of surgical procedure: ORP vs RARP.
Three outcomes within 1 year after the inpatient prostatectomy were investigated: (1) total health care costs, including reimbursement paid by insurers and out of pocket by patients; (2) health care use, including inpatient readmission, emergency department, hospital outpatient, and office visits; and (3) estimated days missed from work due to health care use.
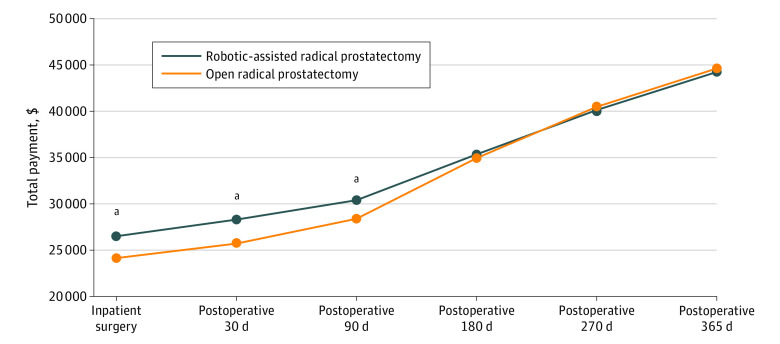
Of the 11 457 patients who underwent inpatient prostatectomy, 1604 (14.0%) had ORP and 9853 (86.0%) had RARP and most patients (8467 [73.9%]) were aged 55 to 64 years. Compared with patients who underwent ORP, those who received RARP had a higher cost at the index hospitalization (mean difference, $2367; 95% CI, $1821-$2914; P < .001), but similar total cumulative costs were observed within 180 days (mean difference, $397; 95% CI, -$582 to $1375; P = .43) and 1 year after discharge (-$383; 95% CI, -$1802 to $1037; P = .60). One-year postdischarge health care use was significantly lower in the RARP compared with ORP group for mean numbers of emergency department visits (-0.09 visits; 95% CI, -0.11 to -0.07 visits; P < .001) and hospital outpatient visits (-1.5 visits; -1.63 to -1.36 visits; P < .001). The reduction in use of health care services among patients who underwent RARP translated into additional savings of $2929 (95% CI, $1600-$4257; P < .001) and approximately 1.69 fewer days (95% CI, 1.49-1.89 days; P < .001) missed from work for health care visits.
Total cumulative cost in this study was similar between ORP and RARP 1 year post discharge; this finding suggests that lower postdischarge health care use after RARP may offset the higher costs during the index hospitalization.

随着机器人手术的应用和使用模式的改变以及前列腺癌患者总体生存率的提高,评估前列腺癌患者治疗的即时和长期成本影响变得尤为重要。
比较开放式根治性前列腺切除术(ORP)与机器人辅助根治性前列腺切除术(RARP)治疗前列腺癌患者 1 年后的卫生保健费用和使用情况。
设计、设置和参与者:本回顾性队列研究使用了美国商业索赔数据库,时间范围为 2013 年 1 月 1 日至 2018 年 12 月 31 日。共纳入 11457 名年龄在 18 至 64 岁之间的男性患者,他们因前列腺癌接受了住院根治性前列腺切除术,并且在住院前列腺切除术之前 180 天至之后 365 天期间连续接受了医疗和处方药覆盖。采用逆概率治疗加权分析来检查手术方式对卫生保健服务费用和使用的差异。数据分析于 2019 年 9 月至 2020 年 7 月进行。
手术方式:ORP 与 RARP。
在住院前列腺切除术 1 年内调查了 3 个结果:(1)总卫生保健费用,包括保险公司支付的报销和患者自付费用;(2)卫生保健使用情况,包括住院再入院、急诊、医院门诊和就诊;(3)因卫生保健使用而缺勤的估计天数。
在接受住院前列腺切除术的 11457 名患者中,1604 名(14.0%)接受了 ORP,9853 名(86.0%)接受了 RARP,大多数患者(8467 [73.9%])年龄在 55 至 64 岁之间。与接受 ORP 的患者相比,接受 RARP 的患者在指数住院期间的费用更高(平均差异为 2367 美元;95%CI,1821-2914 美元;P < .001),但在 180 天内(平均差异为 397 美元;95%CI,-582 至 1375 美元;P = .43)和出院后 1 年(平均差异为-383 美元;95%CI,-1802 至-1037 美元;P = .60)的总累计成本相似。RARP 组患者出院后 1 年内急诊就诊(平均减少 0.09 次就诊;95%CI,-0.11 至-0.07 次就诊;P < .001)和医院门诊就诊(平均减少 1.5 次就诊;95%CI,-1.63 至-1.36 次就诊;P < .001)的次数明显低于 ORP 组。RARP 组患者卫生保健服务使用量的减少转化为 2929 美元(95%CI,1600-4257 美元;P < .001)的额外节省和约 1.69 天(95%CI,1.49-1.89 天;P < .001)的缺勤。
出院后 1 年,ORP 和 RARP 的总累计成本相似;这一发现表明,RARP 后较低的出院后卫生保健使用量可能会抵消指数住院期间较高的费用。