USAID/Defeat TB Project, University Research Co. LLC, Kampala, Uganda.
The Infectious Diseases Institute, College of Health Sciences, Makerere University, P.O. Box 22418, Kampala, Uganda.
BMC Infect Dis. 2021 Mar 22;21(1):292. doi: 10.1186/s12879-021-05967-2.
The World Health Organization (WHO) End TB strategy aims to reduce mortality due to tuberculosis (TB) to less than 5% by 2035. However, mortality due to multidrug-resistant tuberculosis (MDR-TB) remains particularly high. Globally, almost 20% of patients started on MDR-TB treatment die during the course of treatment every year. We set out to examine the risk factors for mortality among a cohort of patients diagnosed with MDR-TB in Uganda.
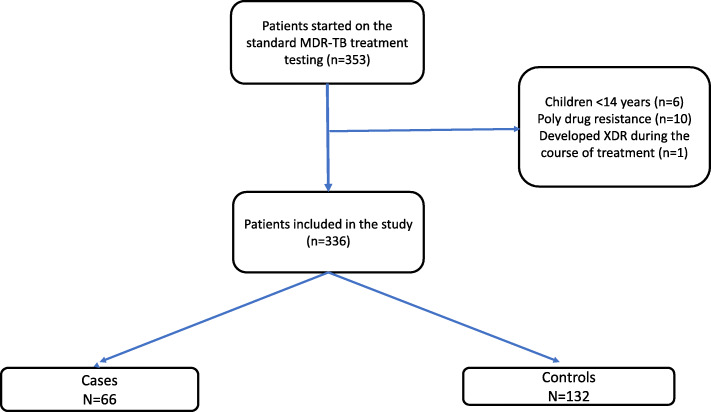
We conducted a case-control study nested within the national MDR-TB cohort. We defined cases as patients who died from any cause during the course of MDR-TB treatment. We selected two controls for each case from patients alive and on MDR-TB treatment at the time that the death occurred (incidence-density sampling). We matched the cases and controls on health facility at which they were receiving care. We performed conditional logistic regression to identify the risk factors for mortality.
Data from 198 patients (66 cases and 132 controls) started on MDR-TB treatment from January 1 to December 31, 2016, was analyzed for this study. Cases were similar to controls in age/sex distribution, occupation and history of TB treatment. However, cases were more likely to be HIV infected while controls were more likely to have attained secondary level education. On multivariate regression analysis, co-infection with HIV (aOR 1.9, 95% CI [1.1-4.92] p = 0.05); non-adherence to MDR-TB treatment (aOR 1.92, 95% CI [1.02-4.83] p = 0.04); age over 50 years (aOR 3.04, 95% CI [1.13-8.20] p = 0.03); and having no education (aOR 3.61, 95% CI [1.1-10.4] p = 0.03) were associated with MDR-TB mortality.
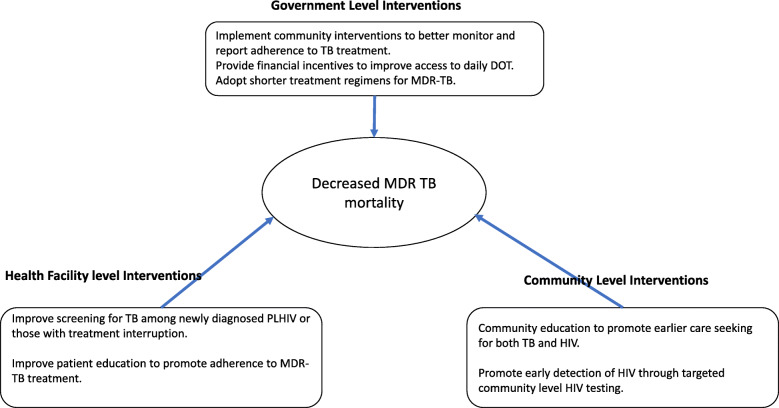
To mitigate MDR-TB mortality, attention must be paid to provision of social support particularly for older persons on MDR-TB treatment. In addition, interventions that support treatment adherence and promote early detection and management of TB among HIV infected persons should also be emphasized.
世界卫生组织(WHO)的终结结核病战略旨在到 2035 年将结核病(TB)死亡率降低到 5%以下。然而,耐多药结核病(MDR-TB)的死亡率仍然特别高。在全球范围内,每年几乎有 20%接受 MDR-TB 治疗的患者在治疗过程中死亡。我们着手研究乌干达 MDR-TB 患者队列中死亡的危险因素。
我们进行了一项嵌套在国家 MDR-TB 队列中的病例对照研究。我们将病例定义为在 MDR-TB 治疗过程中因任何原因死亡的患者。我们从死亡发生时正在接受治疗且存活的患者中为每个病例选择了两个对照(发病率密度抽样)。我们根据接受治疗的医疗机构对病例和对照进行匹配。我们进行了条件逻辑回归以确定死亡的危险因素。
从 2016 年 1 月 1 日至 12 月 31 日开始接受 MDR-TB 治疗的 198 名患者(66 例病例和 132 例对照)的数据用于本研究。病例在年龄/性别分布、职业和结核病治疗史方面与对照相似。然而,病例更有可能感染艾滋病毒,而对照更有可能接受过中等教育。在多变量回归分析中,艾滋病毒合并感染(调整比值比 [aOR] 1.9,95%置信区间 [1.1-4.92],p=0.05);不遵守 MDR-TB 治疗(aOR 1.92,95%CI [1.02-4.83],p=0.04);年龄超过 50 岁(aOR 3.04,95%CI [1.13-8.20],p=0.03);和没有受过教育(aOR 3.61,95%CI [1.1-10.4],p=0.03)与 MDR-TB 死亡率相关。
为了降低 MDR-TB 死亡率,必须注意为接受 MDR-TB 治疗的老年人提供社会支持。此外,还应强调支持治疗依从性和促进 HIV 感染者早期发现和管理结核病的干预措施。