Zhao Peng, Yoo Illhoi, Naqvi Syed H
Institute for Data Science and Informatics, University of Missouri, Columbia, MO, United States.
Department of Health Management and Informatics, School of Medicine, University of Missouri, Columbia, MO, United States.
JMIR Med Inform. 2021 Mar 23;9(3):e16306. doi: 10.2196/16306.
Existing readmission reduction solutions tend to focus on complementing inpatient care with enhanced care transition and postdischarge interventions. These solutions are initiated near or after discharge, when clinicians' impact on inpatient care is ending. Preventive intervention during hospitalization is an underexplored area that holds potential for reducing readmission risk. However, it is challenging to predict readmission risk at the early stage of hospitalization because few data are available.
The objective of this study was to build an early prediction model of unplanned 30-day hospital readmission using a large and diverse sample. We were also interested in identifying novel readmission risk factors and protective factors.
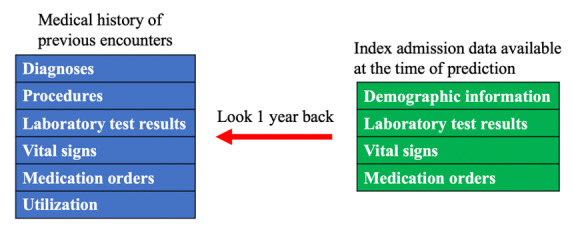
We extracted the medical records of 96,550 patients in 205 participating Cerner client hospitals across four US census regions in 2016 from the Health Facts database. The model was built with index admission data that can become available within 24 hours and data from previous encounters up to 1 year before the index admission. The candidate models were evaluated for performance, timeliness, and generalizability. Multivariate logistic regression analysis was used to identify readmission risk factors and protective factors.
We developed six candidate readmission models with different machine learning algorithms. The best performing model of extreme gradient boosting (XGBoost) achieved an area under the receiver operating characteristic curve of 0.753 on the development data set and 0.742 on the validation data set. By multivariate logistic regression analysis, we identified 14 risk factors and 2 protective factors of readmission that have never been reported.
The performance of our model is better than that of the most widely used models in US health care settings. This model can help clinicians identify readmission risk at the early stage of hospitalization so that they can pay extra attention during the care process of high-risk patients. The 14 novel risk factors and 2 novel protective factors can aid understanding of the factors associated with readmission.
现有的降低再入院率的解决方案往往侧重于通过加强护理过渡和出院后干预来补充住院护理。这些解决方案在出院时或出院后不久启动,此时临床医生对住院护理的影响即将结束。住院期间的预防性干预是一个尚未充分探索的领域,具有降低再入院风险的潜力。然而,由于可用数据较少,在住院早期预测再入院风险具有挑战性。
本研究的目的是使用大量多样的样本建立非计划30天医院再入院的早期预测模型。我们还对识别新的再入院风险因素和保护因素感兴趣。
我们从健康事实数据库中提取了2016年美国四个普查区域205家参与的Cerner客户医院中96550名患者的病历。该模型使用可在24小时内获得的索引入院数据以及索引入院前1年内以前就诊的数据构建。对候选模型的性能、及时性和通用性进行了评估。使用多变量逻辑回归分析来识别再入院风险因素和保护因素。
我们开发了六种具有不同机器学习算法的候选再入院模型。表现最佳的极端梯度提升(XGBoost)模型在开发数据集上的受试者操作特征曲线下面积为0.753,在验证数据集上为0.742。通过多变量逻辑回归分析,我们确定了14个从未报告过再入院的风险因素和2个保护因素。
我们模型的性能优于美国医疗保健环境中使用最广泛的模型。该模型可以帮助临床医生在住院早期识别再入院风险,以便他们在高危患者的护理过程中能够格外关注。这14个新的风险因素和2个新的保护因素有助于理解与再入院相关的因素。