Department of Oncology and Metabolism, University of Sheffield Medical School, Sheffield, UK.
Brighton and Sussex Medical School, Falmer, Brighton, UK.
Br J Surg. 2021 May 27;108(5):499-510. doi: 10.1093/bjs/znab005.
Rates of surgery and adjuvant therapy for breast cancer vary widely between breast units. This may contribute to differences in survival. This cluster RCT evaluated the impact of decision support interventions (DESIs) for older women with breast cancer, to ascertain whether DESIs influenced quality of life, survival, decision quality, and treatment choice.
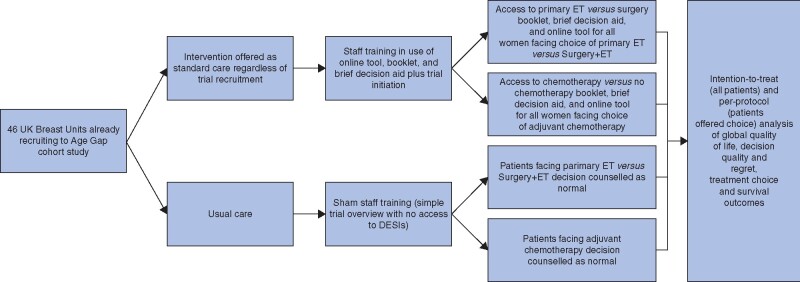
A multicentre cluster RCT compared the use of two DESIs against usual care in treatment decision-making in older women (aged at least ≥70 years) with breast cancer. Each DESI comprised an online algorithm, booklet, and brief decision aid to inform choices between surgery plus adjuvant endocrine therapy versus primary endocrine therapy, and adjuvant chemotherapy versus no chemotherapy. The primary outcome was quality of life. Secondary outcomes included decision quality measures, survival, and treatment choice.
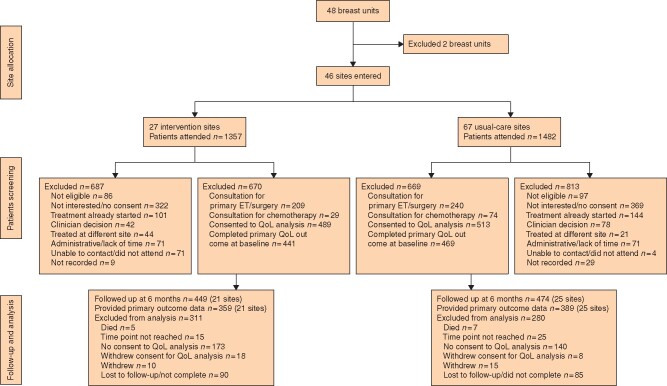
A total of 46 breast units were randomized (21 intervention, 25 usual care), recruiting 1339 women (670 intervention, 669 usual care). There was no significant difference in global quality of life at 6 months after the baseline assessment on intention-to-treat analysis (difference -0.20, 95 per cent confidence interval (C.I.) -2.69 to 2.29; P = 0.900). In women offered a choice of primary endocrine therapy versus surgery plus endocrine therapy, knowledge about treatments was greater in the intervention arm (94 versus 74 per cent; P = 0.003). Treatment choice was altered, with a primary endocrine therapy rate among women with oestrogen receptor-positive disease of 21.0 per cent in the intervention versus 15.4 per cent in usual-care sites (difference 5.5 (95 per cent C.I. 1.1 to 10.0) per cent; P = 0.029). The chemotherapy rate was 10.3 per cent at intervention versus 14.8 per cent at usual-care sites (difference -4.5 (C.I. -8.0 to 0) per cent; P = 0.013). Survival was similar in both arms.
The use of DESIs in older women increases knowledge of breast cancer treatment options, facilitates shared decision-making, and alters treatment selection. Trial registration numbers: EudraCT 2015-004220-61 (https://eudract.ema.europa.eu/), ISRCTN46099296 (http://www.controlled-trials.com).
乳腺癌的手术和辅助治疗率在各乳腺单位之间差异很大。这可能导致生存率的差异。这项聚类 RCT 评估了决策支持干预(DESI)对老年乳腺癌患者的影响,以确定 DESI 是否影响生活质量、生存率、决策质量和治疗选择。
一项多中心聚类 RCT 比较了两种 DESI 与老年乳腺癌患者(年龄至少≥70 岁)治疗决策中的常规护理的使用。每个 DESI 包括一个在线算法、小册子和简短的决策辅助工具,以告知手术加辅助内分泌治疗与原发性内分泌治疗、辅助化疗与无化疗之间的选择。主要结果是生活质量。次要结果包括决策质量测量、生存率和治疗选择。
共有 46 个乳腺单位随机分组(21 个干预组,25 个常规护理组),招募了 1339 名女性(670 名干预组,669 名常规护理组)。意向治疗分析的基线评估后 6 个月的整体生活质量没有显著差异(差异-0.20,95%置信区间(CI)-2.69 至 2.29;P=0.900)。在提供原发性内分泌治疗与手术加内分泌治疗选择的女性中,干预组对治疗的了解程度更高(94%比 74%;P=0.003)。治疗选择发生了改变,在雌激素受体阳性疾病的女性中,接受内分泌治疗的比例在干预组为 21.0%,而常规护理组为 15.4%(差异 5.5(95%CI 1.1 至 10.0)%;P=0.029)。干预组的化疗率为 10.3%,常规护理组为 14.8%(差异-4.5(CI-8.0 至 0)%;P=0.013)。两组的生存率相似。
在老年女性中使用 DESI 增加了对乳腺癌治疗选择的了解,促进了共同决策,并改变了治疗选择。试验注册号:EudraCT 2015-004220-61(https://eudract.ema.europa.eu/),ISRCTN46099296(http://www.controlled-trials.com)。