Gueziri Houssem-Eddine, Rabau Oded, Santaguida Carlo, Collins D Louis
McConnell Brain Imaging Centre, Montreal Neurological Institute and Hospital, McGill University, Montreal, QC, Canada.
Department of Neurology and Neurosurgery, McGill University, Montreal, QC, Canada.
Front Oncol. 2021 Mar 4;11:619204. doi: 10.3389/fonc.2021.619204. eCollection 2021.
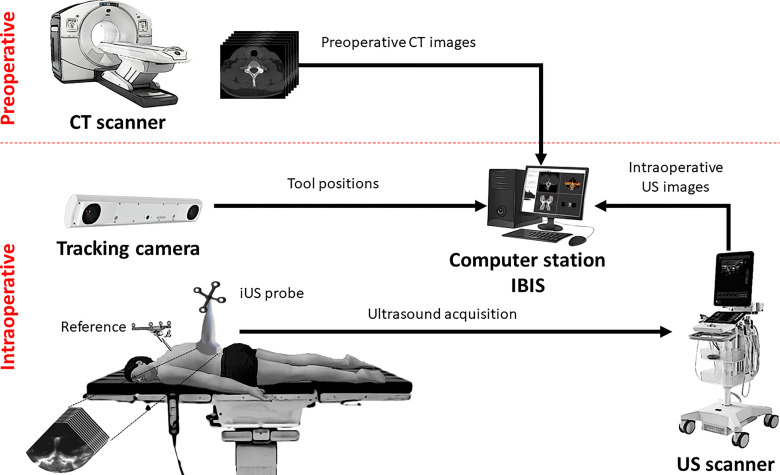
With the growing incidence of patients receiving surgical treatment for spinal metastatic tumours, there is a need for developing cost-efficient and radiation-free alternatives for spinal interventions. In this paper, we evaluate the capabilities and limitations of an image-guided neurosurgery (IGNS) system that uses intraoperative ultrasound (iUS) imaging for guidance.
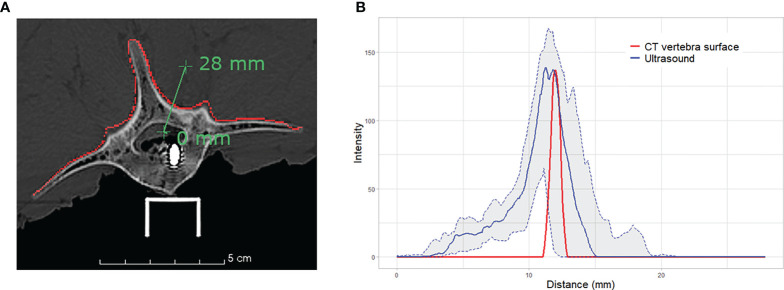
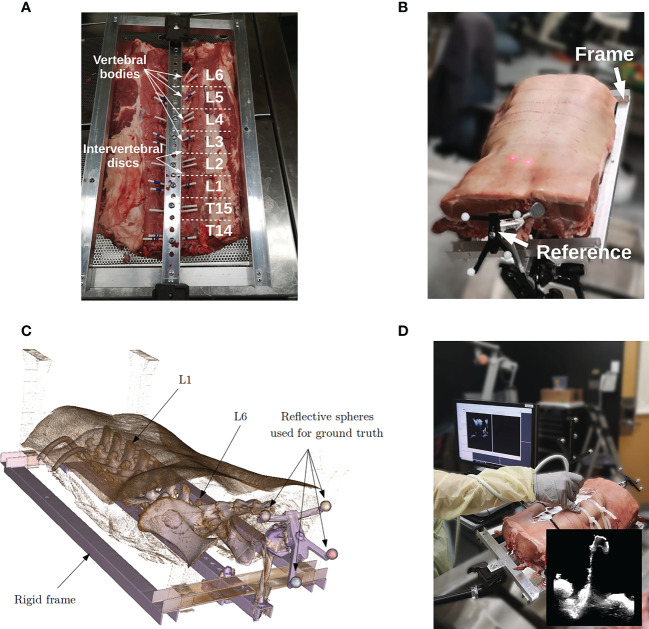
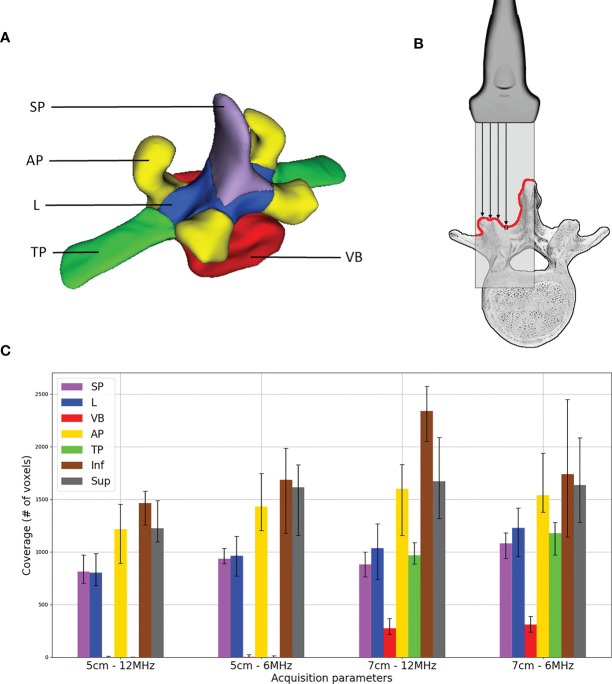
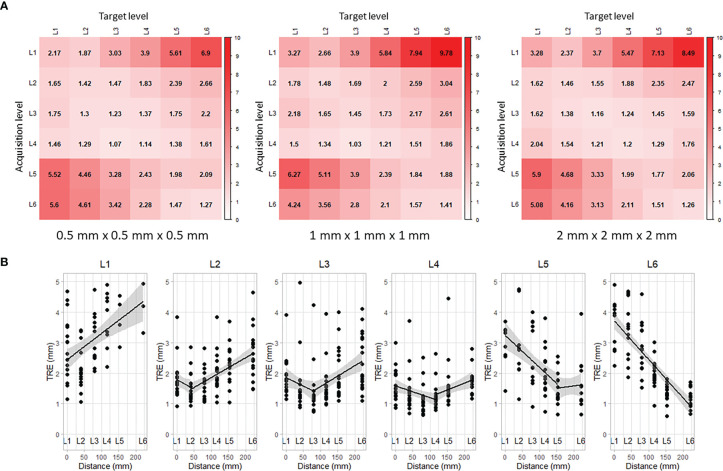
Using a lumbosacral section of a porcine cadaver, we explored the impact of CT image resolution, ultrasound depth and ultrasound frequency on system accuracy, robustness and effectiveness. Preoperative CT images with an isotropic resolution of , and were acquired. During surgery, vertebrae L1 to L6 were exposed. For each vertebra, five iUS scans were acquired using two depth parameters (5 cm and 7 cm) and two frequencies (6 MHz and 12 MHz). A total of 120 acquisition trials were evaluated. Ultrasound-based registration performance is compared to the standard alignment procedure using intraoperative CT. We report target registration error (TRE) and computation time. In addition, the scans' trajectories were analyzed to identify vertebral regions that provide the most relevant features for the alignment.
For all acquisitions, the median TRE ranged from 1.42 mm to 1.58 mm and the overall computation time was 9.04 s ± 1.58 s. Fourteen out of 120 iUS acquisitions (11.66%) yielded a level-to-level mismatch (and these are included in the accuracy measurements reported). No significant effect on accuracy was found with CT resolution ( = 1.70, = 0.232), depth ( = 0.22, = 0.659) nor frequency ( = 1.02, = 0.359). While misalignment increases linearly with the distance from the imaged vertebra, accuracy was satisfactory for directly adjacent levels. A significant relationship was found between iUS scan coverage of laminae and articular processes, and accuracy.
Intraoperative ultrasound can be used for spine surgery neuronavigation. We demonstrated that the IGNS system yield acceptable accuracy and high efficiency compared to the standard CT-based navigation procedure. The flexibility of the iUS acquisitions can have repercussions on the system performance, which are not fully identified. Further investigation is needed to understand the relationship between iUS acquisition and alignment performance.
随着接受脊柱转移性肿瘤手术治疗的患者数量不断增加,需要开发经济高效且无辐射的脊柱干预替代方案。在本文中,我们评估了一种使用术中超声(iUS)成像进行引导的图像引导神经外科手术(IGNS)系统的能力和局限性。
使用猪尸体的腰骶部,我们探讨了CT图像分辨率、超声深度和超声频率对系统准确性、稳健性和有效性的影响。获取了各向同性分辨率为 、 和 的术前CT图像。在手术过程中,暴露L1至L6椎体。对于每个椎体,使用两个深度参数(5厘米和7厘米)和两个频率(6兆赫兹和12兆赫兹)进行五次iUS扫描。共评估了120次采集试验。将基于超声的配准性能与使用术中CT的标准对准程序进行比较。我们报告目标配准误差(TRE)和计算时间。此外,分析扫描轨迹以识别为对准提供最相关特征的椎体区域。
对于所有采集,TRE中位数在1.42毫米至1.58毫米之间,总体计算时间为9.04秒±1.58秒。120次iUS采集中有14次(11.66%)出现层间不匹配(这些包含在报告的准确性测量中)。未发现CT分辨率( = 1.70, = 0.232)、深度( = 0.22, = 0.659)或频率( = 1.02, = 0.359)对准确性有显著影响。虽然错位随与成像椎体的距离线性增加,但直接相邻层面的准确性令人满意。发现iUS对椎板和关节突的扫描覆盖范围与准确性之间存在显著关系。
术中超声可用于脊柱手术神经导航。我们证明,与基于标准CT的导航程序相比,IGNS系统具有可接受的准确性和高效率。iUS采集的灵活性可能会对系统性能产生影响,而这些影响尚未完全明确。需要进一步研究以了解iUS采集与对准性能之间的关系。