Seifert Robert, Schäfers Michael Andreas, Heitplatz Barbara, Kerschke Laura, Riemann Burkhard, Noto Benjamin
Department of Nuclear Medicine, University Hospital Münster, Germany.
Gerhard Domagk Institute of Pathology, University of Münster.
J Nucl Med. 2021 Mar 26;62(12):1702-9. doi: 10.2967/jnumed.121.261898.
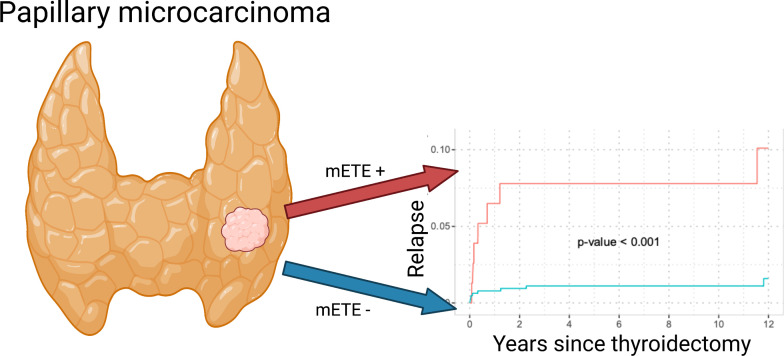
Minimal extrathyroid extension (mETE) is no longer considered in the new 8th edition of the AJCC/UICC staging system. Therefore, papillary thyroid microcarcinoma with mETE previously staged as pT3 will now be staged as pT1a and most likely not receive adjuvant radioiodine therapy. However, it remains unclear if mETE is associated with higher aggressiveness in papillary thyroid microcarcinoma. Therefore, the aim of this study was to investigate if mETE is associated with higher risk of lymph node or distant metastases. 721 patients with thyroid papillary microcarcinoma presenting at our department for postoperative counseling from 05/1983 to 8/2012 were included in this retrospective analysis (median follow-up time 9.30 years). The impact of mETE on the presence of lymph node metastases at thyroidectomy and relapse through lymph node and distant metastases was assessed by logistic regression and Fine-Gray model analyses. 10.7% ( = 77) of patients had mETE. mETE was an independent risk factor for lymph node metastases at thyroidectomy with an adjusted odds ratio of 4.33 (95%CI: 2.02-9.60, p<0.001) in multivariable analysis. Patients with mETE had significantly more relapses through lymph node (over 5 years: 13.1% vs. 1.25%; < 0.001) and distant metastases (over 5 years: 7.8% vs. 1.1%; < 0.001) compared to patients without mETE. mETE was an independent risk factor for relapse through lymph node and distant metastases in multivariable analysis (hazard ratio: 7.78, 95%CI: 2.87-21.16, p< 0.001 and 4.09, 95%CI: 1.25-13.36, = 0.020). mETE is a statistically significant and independent risk factor for relapse through lymph node and distant metastases in papillary microcarcinoma. Therefore, future studies should evaluate, if patients with mETE and microcarcinoma might benefit from intensified surveillance and therapy.
美国癌症联合委员会(AJCC)/国际抗癌联盟(UICC)分期系统的新版第8版不再考虑最小甲状腺外扩展(mETE)。因此,先前分期为pT3的伴有mETE的甲状腺微小乳头状癌现在将分期为pT1a,很可能不会接受辅助放射性碘治疗。然而,mETE是否与甲状腺微小乳头状癌的更高侵袭性相关仍不清楚。因此,本研究的目的是调查mETE是否与更高的淋巴结或远处转移风险相关。本回顾性分析纳入了1983年5月至2012年8月在我科接受术后咨询的721例甲状腺微小乳头状癌患者(中位随访时间9.30年)。通过逻辑回归和Fine-Gray模型分析评估mETE对甲状腺切除时淋巴结转移的存在以及通过淋巴结和远处转移复发的影响。10.7%(n = 77)的患者有mETE。在多变量分析中,mETE是甲状腺切除时淋巴结转移的独立危险因素,调整后的优势比为4.33(95%CI:2.02 - 9.60,p < 0.001)。与无mETE的患者相比,有mETE的患者通过淋巴结复发(超过5年:13.1%对1.25%;p < 0.001)和远处转移(超过5年:7.8%对1.1%;p < 0.001)明显更多。在多变量分析中,mETE是通过淋巴结和远处转移复发的独立危险因素(风险比:7.78,95%CI:2.87 - 21.16,p < 0.001和4.09,95%CI:1.25 - 13.36,p = 0.020)。mETE是甲状腺微小乳头状癌通过淋巴结和远处转移复发的统计学显著且独立的危险因素。因此,未来的研究应评估伴有mETE的微小癌患者是否可能从强化监测和治疗中获益。