Duke Center for Antimicrobial Stewardship and Infection Prevention, Duke University Medical Center, Durham, North Carolina.
Duke Clinical Research Institute, Durham, North Carolina.
JAMA Netw Open. 2021 Mar 1;4(3):e213460. doi: 10.1001/jamanetworkopen.2021.3460.
Comparisons of antimicrobial use among hospitals are difficult to interpret owing to variations in patient case mix. Risk-adjustment strategies incorporating larger numbers of variables haves been proposed as a method to improve comparisons for antimicrobial stewardship assessments.
To evaluate whether variables of varying complexity and feasibility of measurement, derived retrospectively from the electronic health records, accurately identify inpatient antimicrobial use.
DESIGN, SETTING, AND PARTICIPANTS: Retrospective cohort study, using a 2-stage random forests machine learning modeling analysis of electronic health record data. Data were split into training and testing sets to measure model performance using area under the curve and absolute error. All adult and pediatric inpatient encounters from October 1, 2015, to September 30, 2017, at 2 community hospitals and 1 academic medical center in the Duke University Health System were analyzed. A total of 204 candidate variables were categorized into 4 tiers based on feasibility of measurement from the electronic health records.
Antimicrobial exposure was measured at the encounter level in 2 ways: binary (ever or never) and number of days of therapy. Analyses were stratified by age (pediatric or adult), unit type, and antibiotic group.
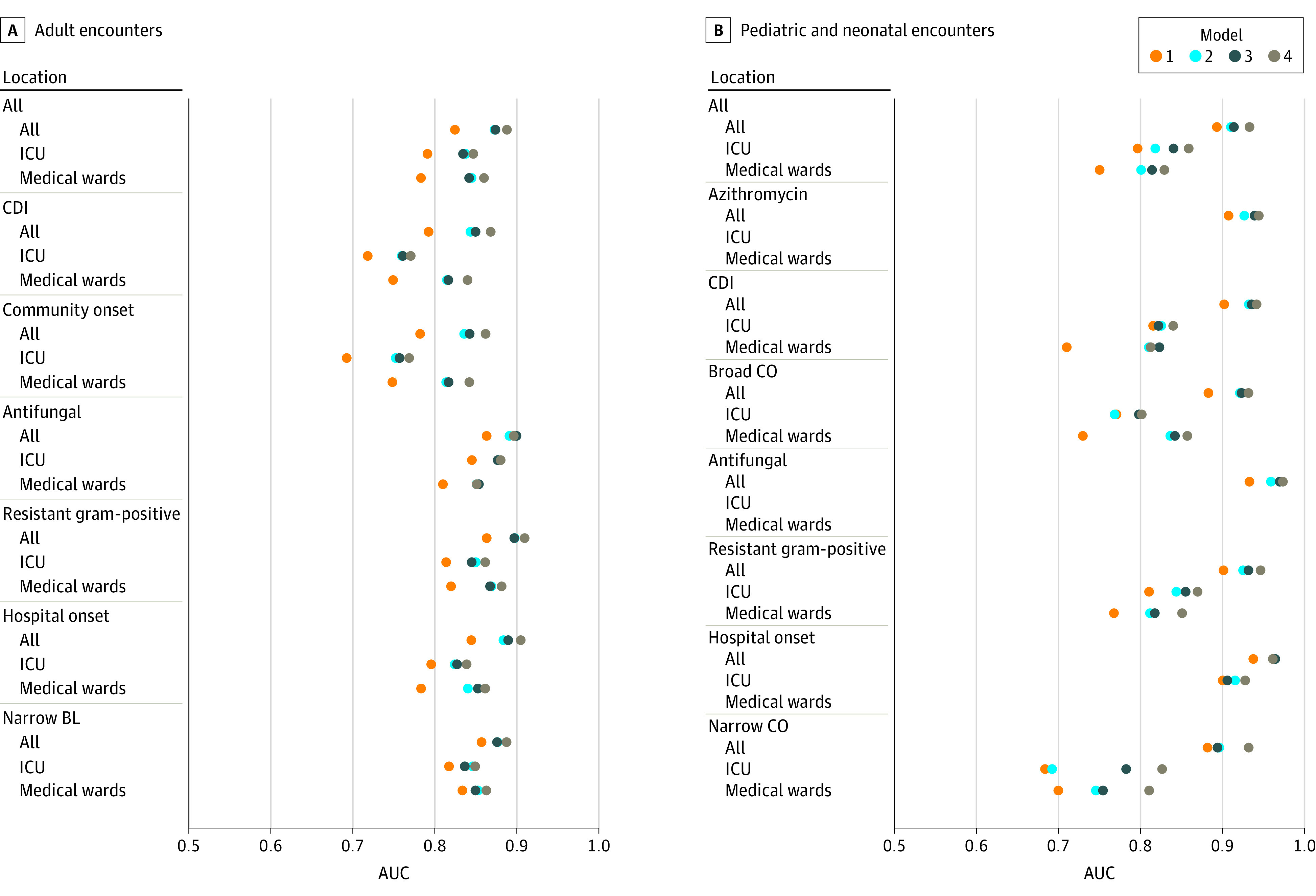
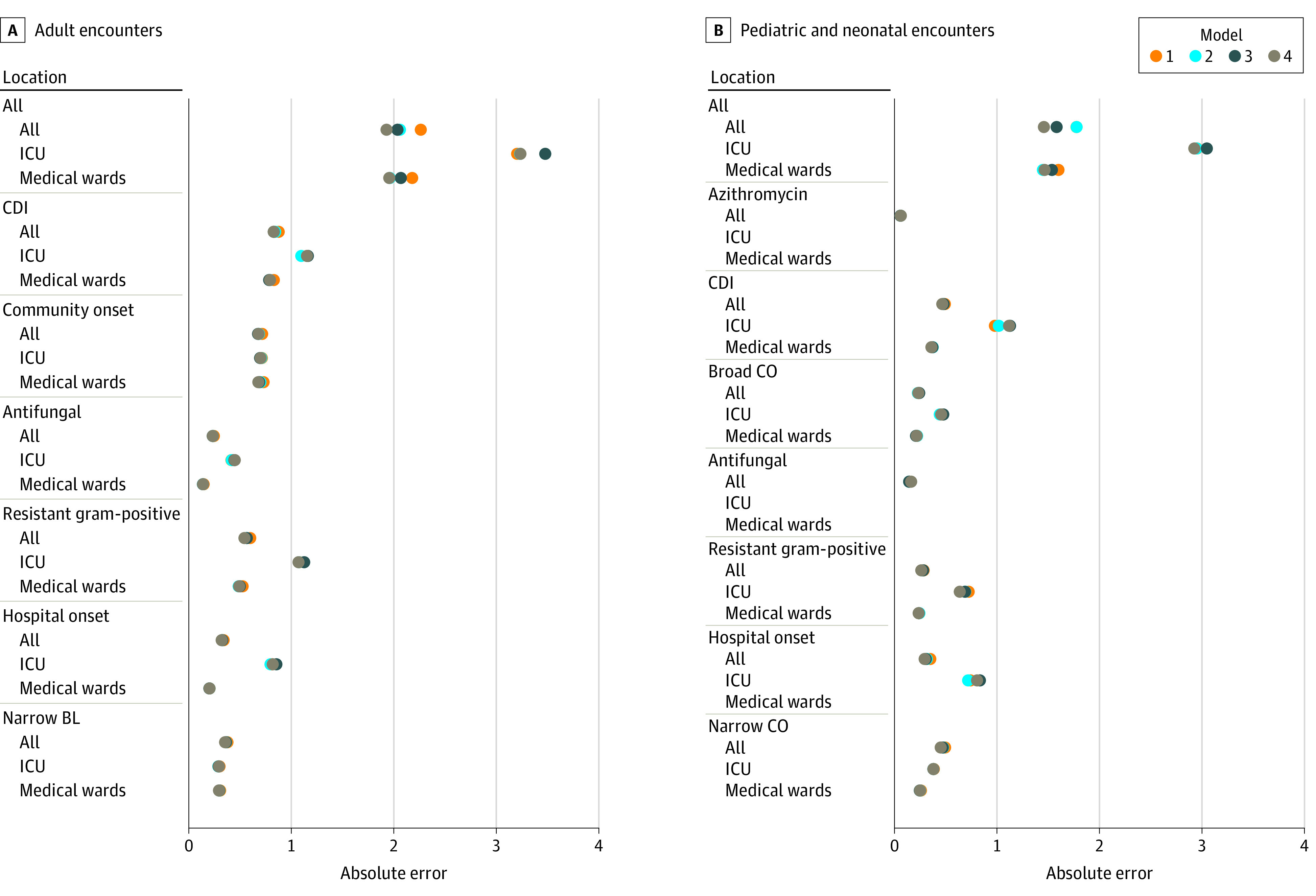
The data set included 170 294 encounters and 204 candidate variables from 3 hospitals during the 3-year study period. Antimicrobial exposure occurred in 80 190 encounters (47%); 64 998 (38%) received 1 to 6 days of therapy, and 15 192 (9%) received 7 or more days of therapy. Two-stage models identified antimicrobial use with high fidelity (mean area under the curve, 0.85; mean absolute error, 1.0 days of therapy). Addition of more complex variables increased accuracy, with largest improvements occurring with inclusion of diagnosis information. Accuracy varied based on location and antibiotic group. Models underestimated the number of days of therapy of encounters with long lengths of stay.
Models using variables derived from electronic health records identified antimicrobial exposure accurately. Future risk-adjustment strategies incorporating encounter-level information may make comparisons of antimicrobial use more meaningful for hospital antimicrobial stewardship assessments.
由于患者病例组合的差异,医院之间的抗菌药物使用情况比较难以解释。已经提出了纳入更多变量的风险调整策略,作为提高抗菌药物管理评估比较的一种方法。
评估从电子健康记录中回顾性获得的复杂程度和可测量性不同的变量是否能准确识别住院患者的抗菌药物使用情况。
设计、地点和参与者:这是一项回顾性队列研究,使用电子健康记录数据的两阶段随机森林机器学习建模分析。数据被分为训练集和测试集,使用曲线下面积和绝对误差来衡量模型性能。所有 2015 年 10 月 1 日至 2017 年 9 月 30 日期间,杜克大学卫生系统的 2 家社区医院和 1 家学术医疗中心的成年和儿科住院患者的所有就诊记录都进行了分析。共有 204 个候选变量根据从电子健康记录中获取的可行性分为 4 个层次。
抗菌药物暴露在就诊水平上以 2 种方式进行测量:二进制(使用或未使用)和治疗天数。分析按年龄(儿科或成人)、病房类型和抗生素组进行分层。
在 3 年的研究期间,该数据集包括来自 3 家医院的 170294 次就诊记录和 204 个候选变量。抗菌药物暴露发生在 80190 次就诊中(47%);64998 次(38%)接受 1-6 天的治疗,15192 次(9%)接受 7 天或以上的治疗。两阶段模型以高保真度识别了抗菌药物的使用(平均曲线下面积为 0.85;平均治疗天数的绝对误差为 1.0 天)。增加更复杂的变量可以提高准确性,最大的改进出现在纳入诊断信息时。准确性因位置和抗生素组而异。对于住院时间较长的就诊,模型低估了治疗天数。
使用电子健康记录中提取的变量建立的模型可以准确地识别抗菌药物的使用情况。未来纳入就诊水平信息的风险调整策略可能会使医院抗菌药物管理评估中的抗菌药物使用比较更有意义。