Department of Neurology and Neurological Sciences, Stanford University School of Medicine, Stanford, CA, 94305, USA.
Department of Radiology, Stanford University Medical Center, Stanford, CA, 94305, USA.
Neurotherapeutics. 2021 Apr;18(2):1039-1063. doi: 10.1007/s13311-021-01023-8. Epub 2021 Mar 30.
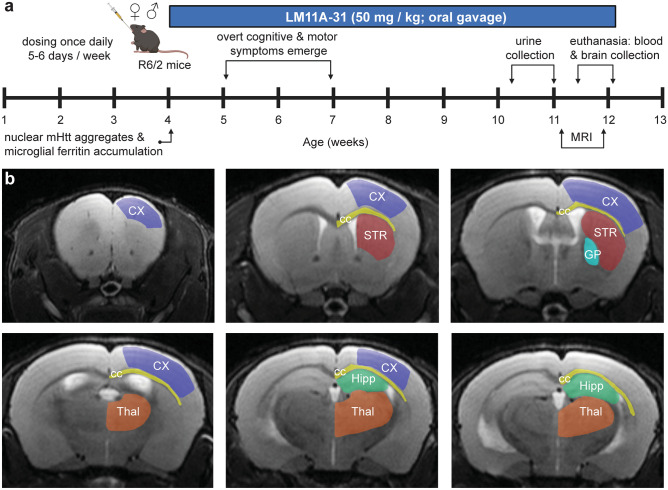
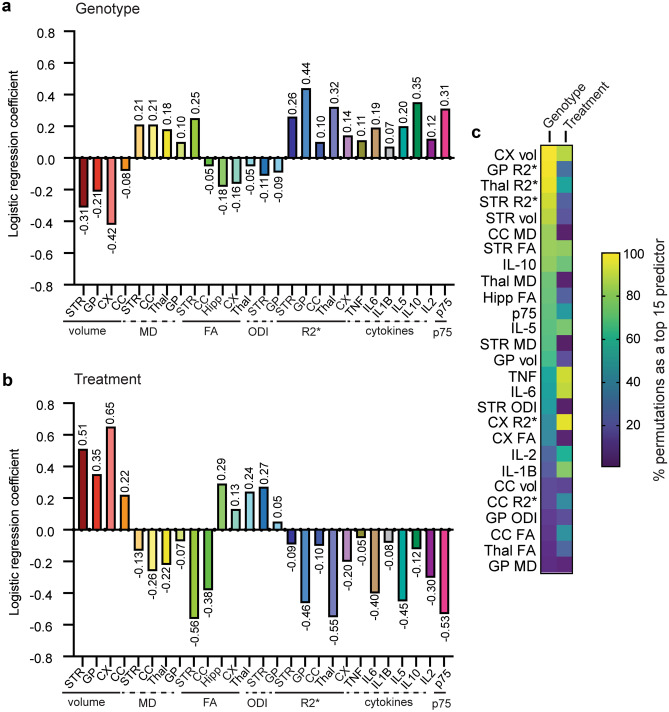
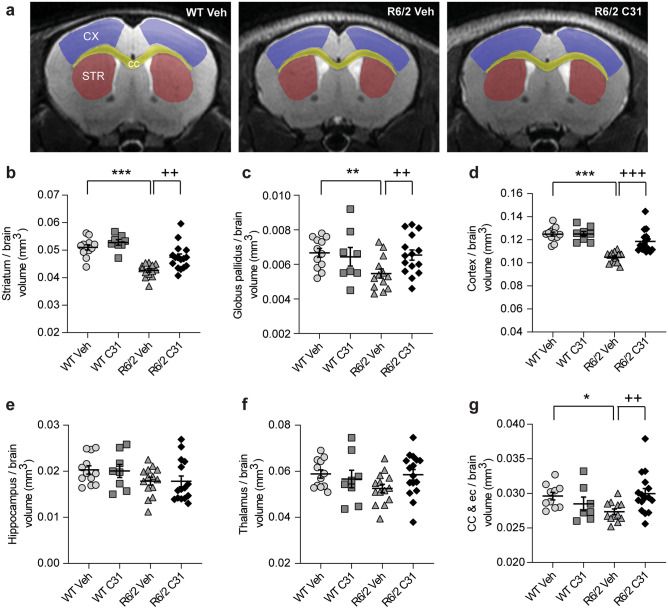
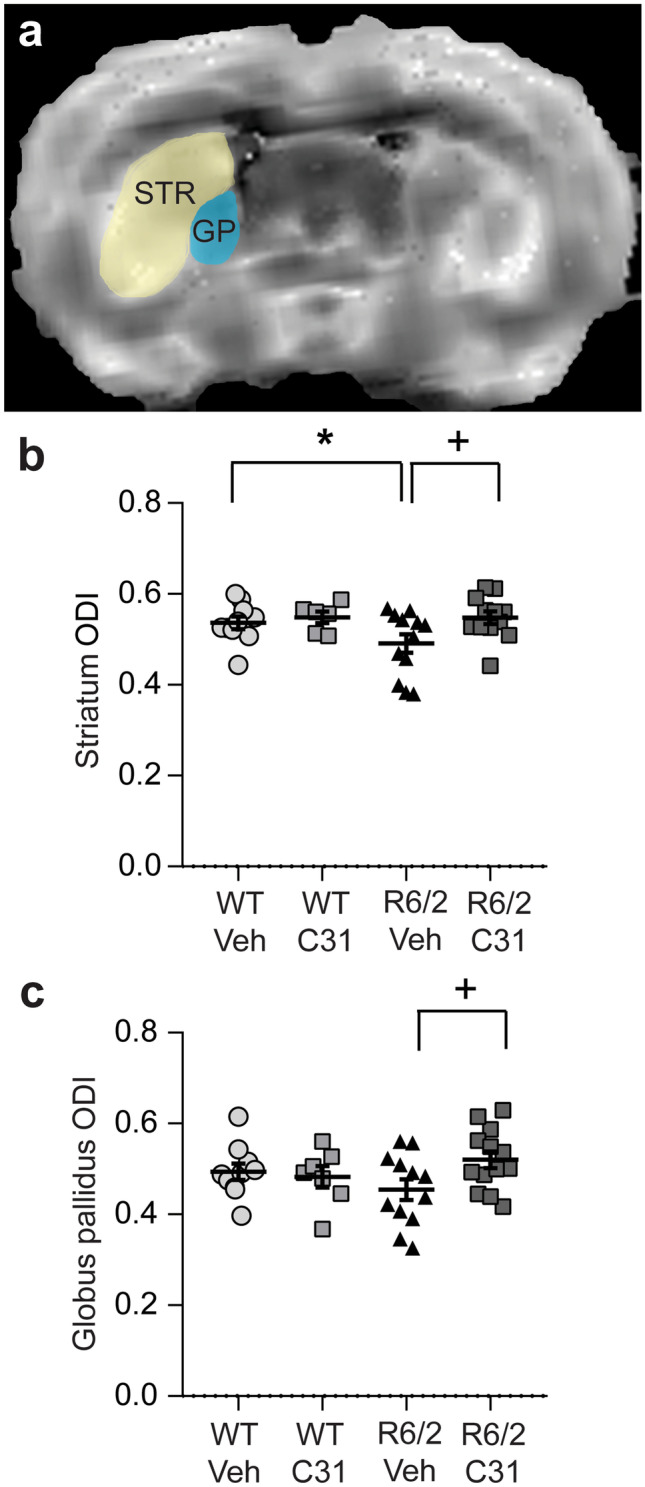
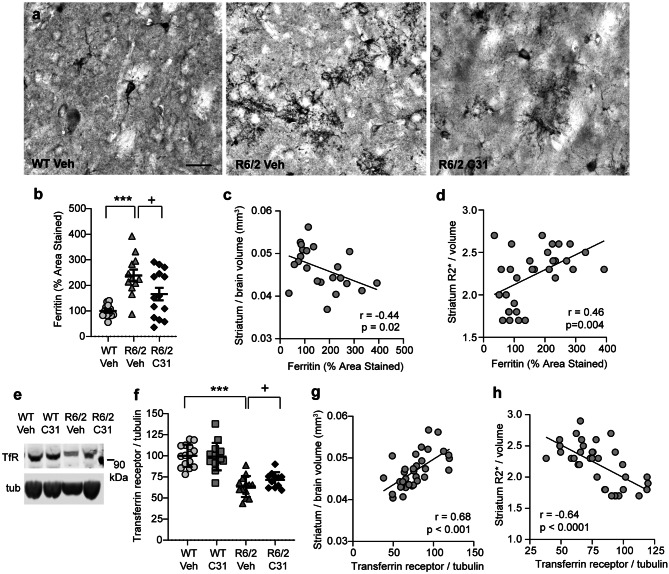
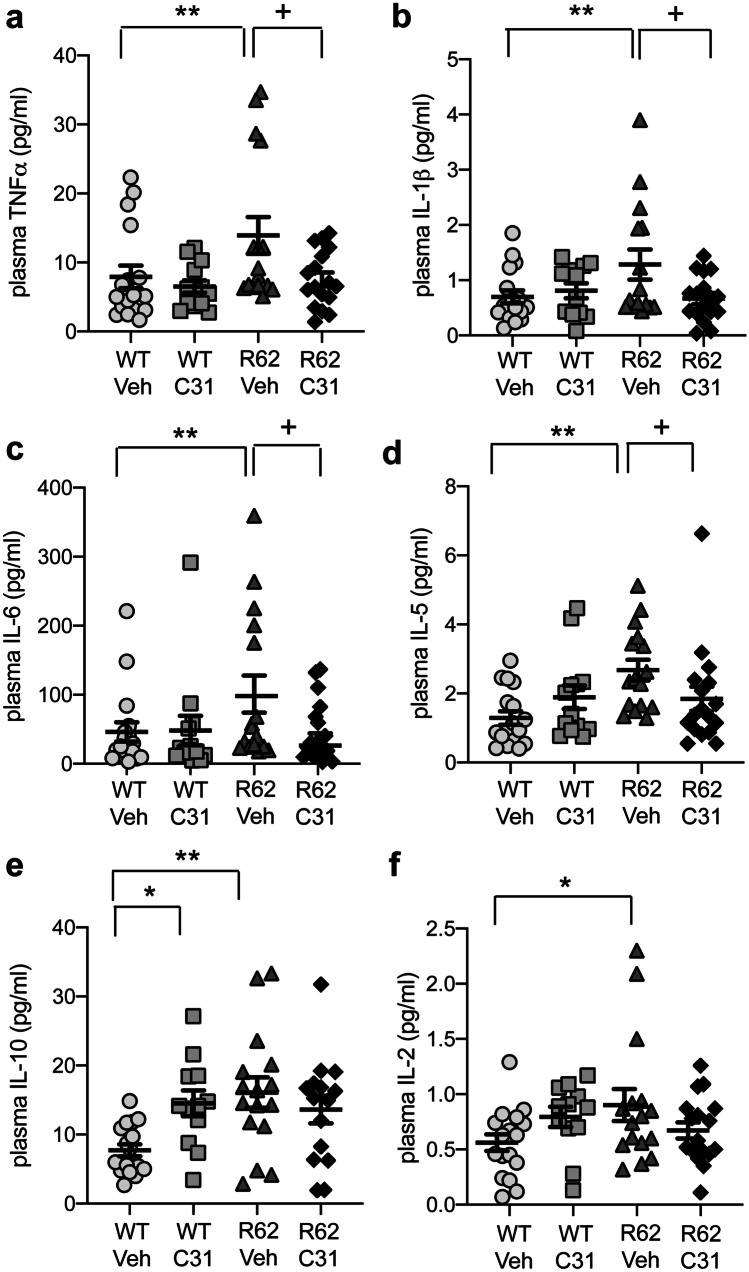
Huntington's disease (HD) is caused by an expansion of the CAG repeat in the huntingtin gene leading to preferential neurodegeneration of the striatum. Disease-modifying treatments are not yet available to HD patients and their development would be facilitated by translatable pharmacodynamic biomarkers. Multi-modal magnetic resonance imaging (MRI) and plasma cytokines have been suggested as disease onset/progression biomarkers, but their ability to detect treatment efficacy is understudied. This study used the R6/2 mouse model of HD to assess if structural neuroimaging and biofluid assays can detect treatment response using as a prototype the small molecule p75 ligand LM11A-31, shown previously to reduce HD phenotypes in these mice. LM11A-31 alleviated volume reductions in multiple brain regions, including striatum, of vehicle-treated R6/2 mice relative to wild-types (WTs), as assessed with in vivo MRI. LM11A-31 also normalized changes in diffusion tensor imaging (DTI) metrics and diminished increases in certain plasma cytokine levels, including tumor necrosis factor-alpha and interleukin-6, in R6/2 mice. Finally, R6/2-vehicle mice had increased urinary levels of the p75 extracellular domain (ecd), a cleavage product released with pro-apoptotic ligand binding that detects the progression of other neurodegenerative diseases; LM11A-31 reduced this increase. These results are the first to show that urinary p75-ecd levels are elevated in an HD mouse model and can be used to detect therapeutic effects. These data also indicate that multi-modal MRI and plasma cytokine levels may be effective pharmacodynamic biomarkers and that using combinations of these markers would be a viable and powerful option for clinical trials.
亨廷顿病(HD)是由亨廷顿基因中的 CAG 重复扩展引起的,导致纹状体的神经退行性变优先发生。目前还没有针对 HD 患者的治疗方法,而这些治疗方法的开发将得益于可转化的药效动力学生物标志物。多模态磁共振成像(MRI)和血浆细胞因子已被提议作为疾病发病/进展的生物标志物,但它们检测治疗效果的能力尚未得到充分研究。本研究使用 R6/2 亨廷顿病小鼠模型来评估结构神经影像学和生物流体分析是否可以使用小分子 p75 配体 LM11A-31 检测治疗反应,该配体先前已被证明可减轻这些小鼠的 HD 表型。LM11A-31 减轻了载药处理的 R6/2 小鼠相对于野生型(WT)的多个脑区(包括纹状体)的体积减少,这是通过体内 MRI 评估的。LM11A-31 还使 DTI 指标的变化正常化,并减少了某些血浆细胞因子水平的升高,包括肿瘤坏死因子-α和白细胞介素-6,在 R6/2 小鼠中。最后,R6/2-载药小鼠的尿 p75 细胞外结构域(ecd)水平升高,这是一种与促凋亡配体结合释放的裂解产物,可检测其他神经退行性疾病的进展;LM11A-31 降低了这种增加。这些结果是首次表明尿 p75-ecd 水平在 HD 小鼠模型中升高,并可用于检测治疗效果。这些数据还表明,多模态 MRI 和血浆细胞因子水平可能是有效的药效动力学生物标志物,并且使用这些标志物的组合将是临床试验的可行和强大选择。