Lindemann Kristina, Smogeli Elisabeth, Småstuen Milada Cvancarova, Bruheim Kjersti, Trovik Jone, Nordberg Terje, Kristensen Gunnar B, Werner Henrica M J, Nakken Esten
Department of Gynecological Oncology, Division of Cancer Medicine, Oslo University Hospital, PB 4953 Nydalen, 0424 Oslo, Norway.
Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, P.O. Box 1171 Blindern, 0318 Oslo, Norway.
Cancers (Basel). 2021 Mar 18;13(6):1367. doi: 10.3390/cancers13061367.
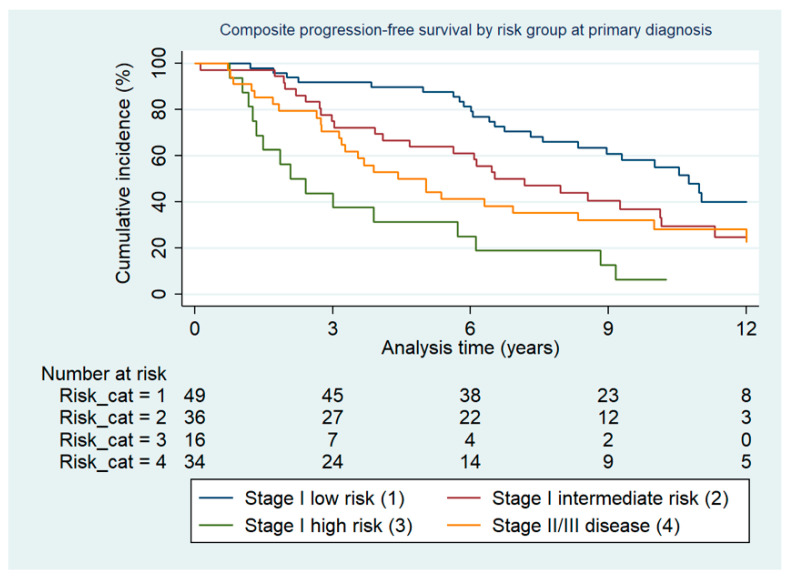
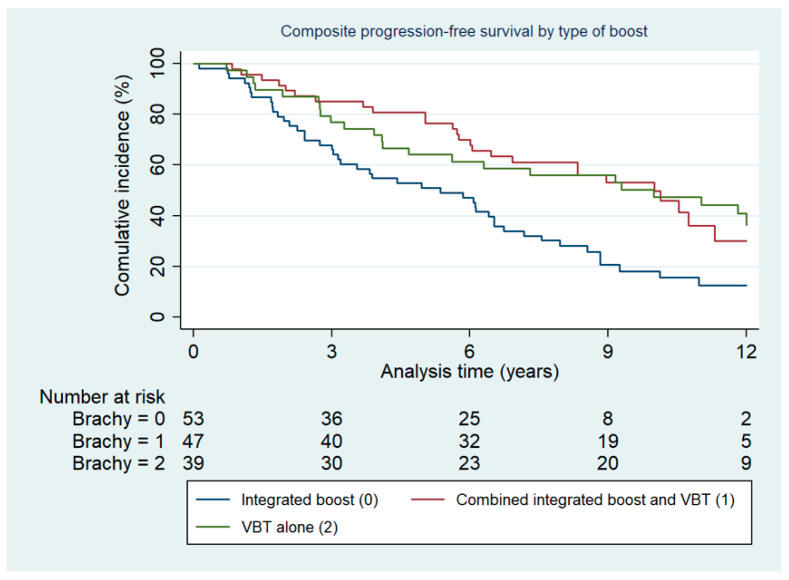
(1) : This study evaluated the clinical outcome after salvage radiotherapy for first pelvic relapse after endometrial cancer (EC). (2) : This multicenter retrospective study included EC patients with first central pelvic relapse without lymph node involvement treated with curative intent. Progression-free (PFS) and overall survival (OS) were calculated with the Kaplan-Meier method and possible predictive factors for risk of relapse and mortality were identified using the Cox model. (3) : We included 139 patients with median EQD2 (Equivalent Dose in 2 Gy fractions) to the clinical target volume of 70.0 Gy. During follow up of median 6.66 years, 39.6% patients developed a second relapse. Risk group classification at primary diagnosis based on histology, grading and FIGO stage and how the pelvic tumor boost was administered were independently associated with PFS and OS. Five-year OS was 68% (95% CI (59-75)) for the whole cohort. Five-year OS was 88% (95% CI (75-94)), 72% (95% CI (55-84)) and 38% (95% CI (15-60)) for the stage I low-, intermediate- and high-risk group, respectively. (4) : The majority of central pelvic recurrences in RT-naive EC women can be successfully salvaged with radiotherapy. However, survival in patients with high-risk disease remains poor and warrants a more individualized approach to optimize outcome.
(1):本研究评估了子宫内膜癌(EC)首次盆腔复发后挽救性放疗的临床结局。(2):这项多中心回顾性研究纳入了有治愈意向且首次盆腔中央复发且无淋巴结受累的EC患者。采用Kaplan-Meier方法计算无进展生存期(PFS)和总生存期(OS),并使用Cox模型确定复发和死亡风险的可能预测因素。(3):我们纳入了139例患者,临床靶区的中位等效剂量(2Gy分割剂量)为70.0Gy。在中位6.66年的随访期间,39.6%的患者出现了第二次复发。基于组织学、分级和国际妇产科联盟(FIGO)分期的初次诊断时的风险组分类以及盆腔肿瘤增敏的给药方式与PFS和OS独立相关。整个队列的5年总生存率为68%(95%置信区间(59 - 75))。I期低、中、高危组的5年总生存率分别为88%(95%置信区间(75 - 94))、72%(95%置信区间(55 - 84))和38%(95%置信区间(15 - 60))。(4):大多数未接受过放疗的EC女性盆腔中央复发可以通过放疗成功挽救。然而,高危疾病患者的生存率仍然很低,需要更个体化的方法来优化结局。