Zhu Guangsheng, Ren Dian, Lei Xi, Shi Ruifeng, Zhu Shuai, Zhou Ning, Zu Lingling, Mello Ramon Andrade De, Chen Jun, Xu Song
Department of Lung Cancer Surgery, Tianjin Medical University General Hospital, Tianjin 300050, China.
Tianjin Key Laboratory of Lung Cancer Metastasis and Tumor Microenvironment, Lung Cancer Institute, Tianjin Medical University General Hospital, Tianjin 300050, China.
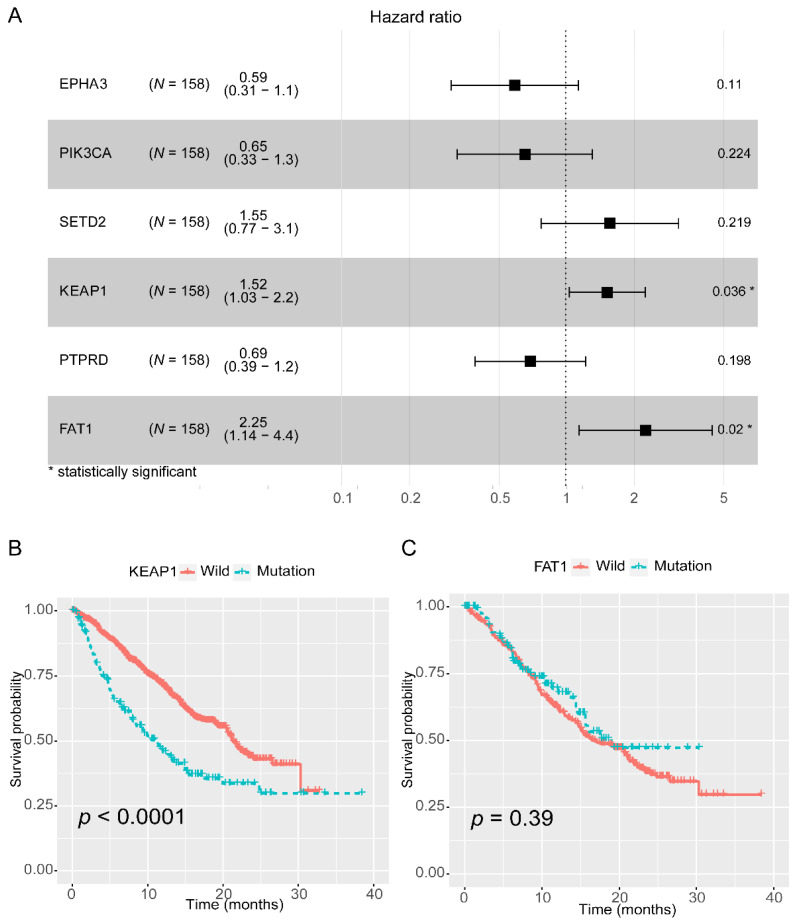
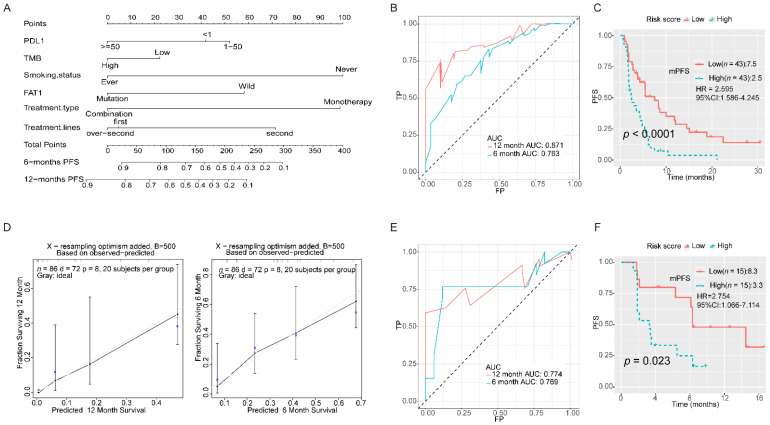
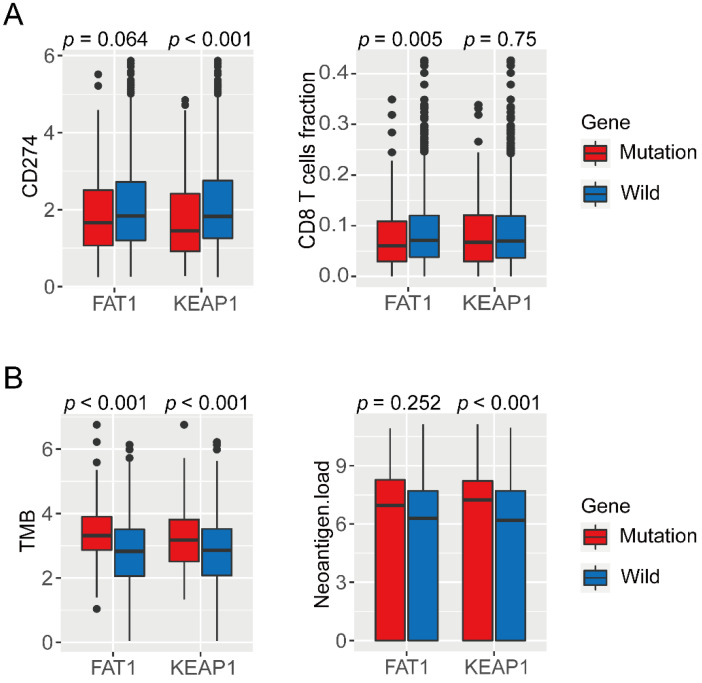
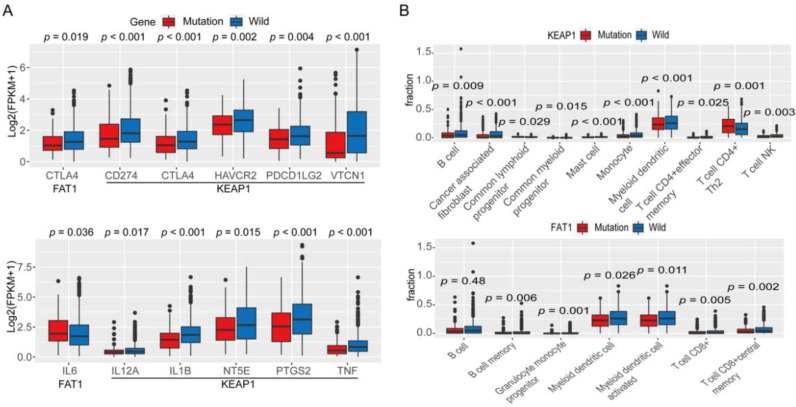
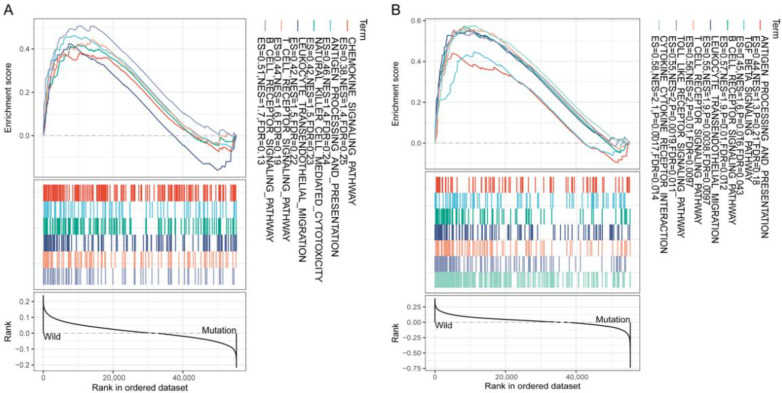
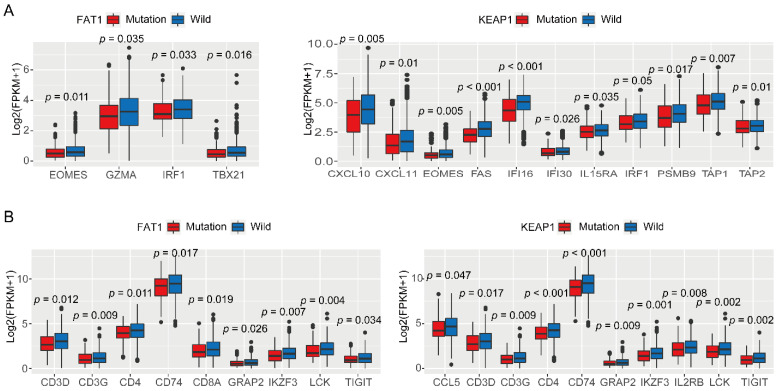
Cancers (Basel). 2021 Mar 19;13(6):1397. doi: 10.3390/cancers13061397.
(1) Background: The immune checkpoint blockade (ICB) has shown promising efficacy in non-small-cell lung cancer (NSCLC) patients with significant clinical benefits and durable responses, but the overall response rate to ICBs is only 20%. The lack of responsiveness to ICBs is currently a central problem in cancer immunotherapy. (2) Methods: Four public cohorts comprising 2986 patients with NSCLC were included in the study. We screened 158 patients with NSCLC with no durable clinical benefit (NDB) to ICBs in the Rizvi cohort and identified NDB-related gene mutations in these patients using univariate and multivariate Cox regression analyses. Programmed death-ligand 1 (PD-L1) expression, tumor mutation burden (TMB), neoantigen load, tumor-infiltrating lymphocytes, and immune-related gene expression were analyzed for identifying gene mutations. A comprehensive predictive classifier model was also built to evaluate the efficacy of ICB therapy. (3) Results: Mutations in FAT1 and KEAP1 were found to correlate with NDB in patients with NSCLC to ICBs; however, the analysis suggested that only mutation in FAT1 was valuable in predicting the efficacy of ICB therapy, and that mutation in KEAP1 acted as a prognostic but not a predictive biomarker for NSCLC. Mutations in FAT1 were associated with a higher TMB and lower multiple lymphocyte infiltration, including CD8 (T-Cell Surface Glycoprotein CD8)+ T cells. We established a prognostic model according to PD-L1 expression, TMB, smoking status, treatment regimen, treatment type, and FAT1 mutation, which indicated good accuracy by receiver operating characteristic (ROC) analysis (area under the curve (AUC) for 6-months survival: 0.763; AUC for 12-months survival: 0.871). (4) Conclusions: Mutation in FAT1 may be a predictive biomarker in patients with NSCLC who exhibit NDB to ICBs. We proposed an FAT1 mutation-based model for screening more suitable NSCLC patients to receive ICBs that may contribute to individualized immunotherapy.
(1) 背景:免疫检查点阻断(ICB)在非小细胞肺癌(NSCLC)患者中显示出有前景的疗效,具有显著的临床益处和持久反应,但ICB的总体反应率仅为20%。对ICB缺乏反应性是目前癌症免疫治疗中的一个核心问题。(2) 方法:该研究纳入了四个包含2986例NSCLC患者的公共队列。我们在Rizvi队列中筛选了158例对ICB无持久临床益处(NDB)的NSCLC患者,并使用单变量和多变量Cox回归分析确定这些患者中与NDB相关的基因突变。分析程序性死亡配体1(PD-L1)表达、肿瘤突变负担(TMB)、新抗原负荷、肿瘤浸润淋巴细胞和免疫相关基因表达以识别基因突变。还构建了一个综合预测分类模型来评估ICB治疗的疗效。(3) 结果:发现FAT1和KEAP1的突变与NSCLC患者对ICB的NDB相关;然而,分析表明只有FAT1突变在预测ICB治疗疗效方面有价值,而KEAP1突变是NSCLC的一个预后生物标志物而非预测生物标志物。FAT1突变与更高的TMB和更低的多种淋巴细胞浸润相关,包括CD8(T细胞表面糖蛋白CD8)+ T细胞。我们根据PD-L1表达、TMB、吸烟状态、治疗方案、治疗类型和FAT1突变建立了一个预后模型,通过受试者操作特征(ROC)分析显示出良好的准确性(6个月生存率的曲线下面积(AUC):0.763;12个月生存率的AUC:0.871)。(4) 结论:FAT1突变可能是对ICB表现出NDB的NSCLC患者的一个预测生物标志物。我们提出了一个基于FAT1突变的模型,用于筛选更适合接受ICB的NSCLC患者,这可能有助于个性化免疫治疗。