Singh Sunny R K, Malapati Sindhu J, Kumar Rohit, Willner Christopher, Wang Ding
Henry Ford Cancer Institute, Henry Ford Health System, Detroit, MI 48202, USA.
Department of Hematology and Oncology, Ascension St John Hospital, Detroit, MI 48236, USA.
Cancers (Basel). 2021 Mar 22;13(6):1455. doi: 10.3390/cancers13061455.
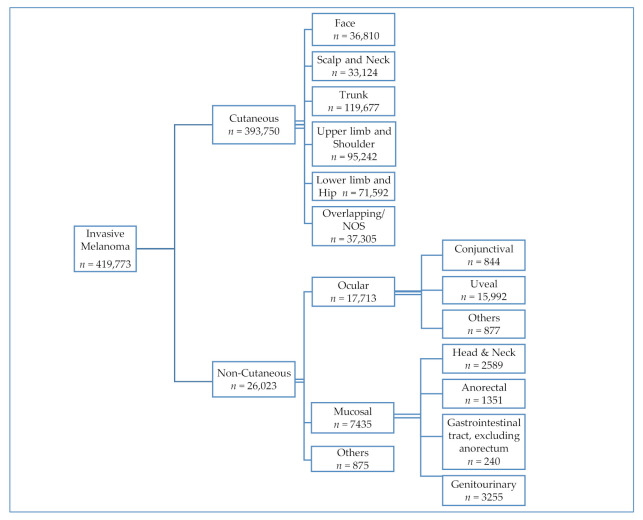
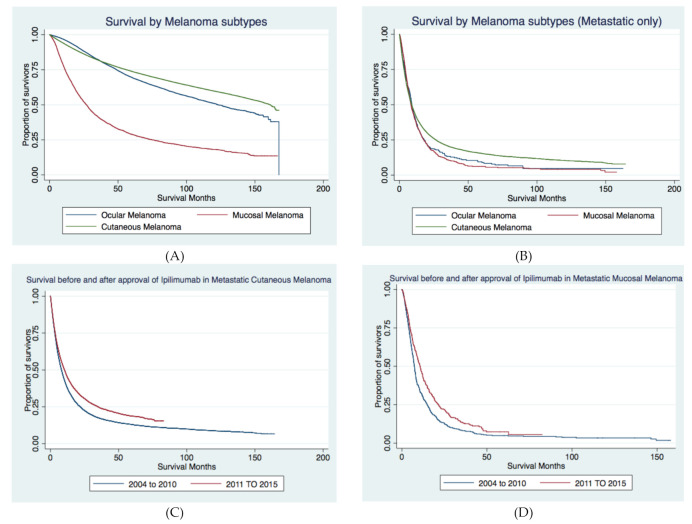
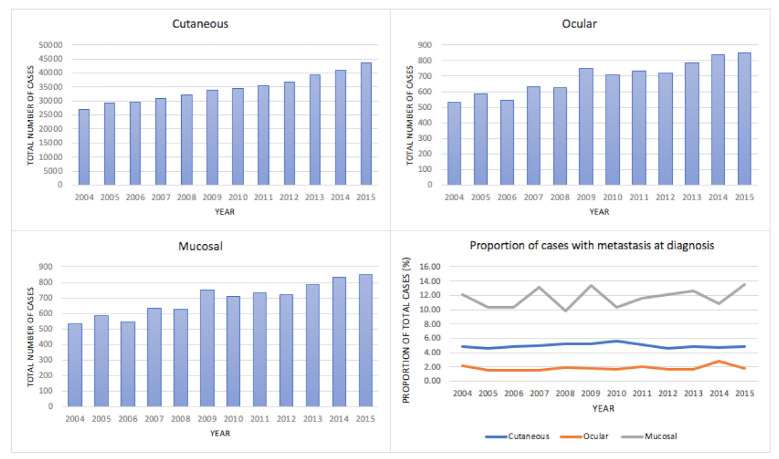
The incidence of invasive melanoma is rising, and approval for the first immune checkpoint inhibitor (ICI) to treat metastatic melanoma occurred in 2011. We aim to describe the epidemiology and outcomes in recent years, sociodemographic factors associated with the presence of metastasis at diagnosis, and the real-world impact of ICI approval on survival based on melanoma subtype and race. This is a retrospective analysis of the National Cancer Database (NCDB) from the years 2004-2015. The primary outcome was the overall survival of metastatic melanoma by subtype. Secondary outcomes included sociodemographic factors associated with the presence of metastasis at diagnosis and the impact of treatment facility type and ICI approval on the survival of metastatic melanoma. Of the 419,773 invasive melanoma cases, 93.80% were cutaneous, and 4.92% were metastatic at presentation. The odds of presenting with metastatic disease were higher in African Americans (AA) compared to Caucasians (OR 2.37; 95% CI 2.11-2.66, < 0.001). Treatment of metastatic melanoma at an academic/research facility was associated with lower mortality versus community cancer programs (OR 0.75, 95 % CI 0.69-0.81, -value < 0.001). Improvement in survival of metastatic melanoma was noted for Caucasians after the introduction of ICI (adjusted HR 0.80, 95% CI 0.78-0.83, < 0.001); however, this was not statistically significant for AA (adjusted HR 0.80, 95% CI 0.62-1.02, -value = 0.073) or ocular cases (HR 1.03, 95% CI 0.81-1.31, -value = 0.797). Real-world data suggest a 20% improvement in survival of metastatic melanoma since the introduction of ICI. The disproportionately high odds of metastatic disease at presentation in AA patients with melanoma suggest the need for a better understanding of the disease and improvement in care delivery.
侵袭性黑色素瘤的发病率正在上升,2011年首个用于治疗转移性黑色素瘤的免疫检查点抑制剂(ICI)获得批准。我们旨在描述近年来的流行病学和治疗结果、诊断时与转移存在相关的社会人口学因素,以及ICI批准对基于黑色素瘤亚型和种族的生存的实际影响。这是一项对2004年至2015年国家癌症数据库(NCDB)的回顾性分析。主要结局是按亚型划分的转移性黑色素瘤的总生存期。次要结局包括与诊断时转移存在相关的社会人口学因素,以及治疗机构类型和ICI批准对转移性黑色素瘤生存的影响。在419773例侵袭性黑色素瘤病例中,93.80%为皮肤型,4.92%在初诊时为转移性。与白种人相比,非裔美国人(AA)初诊时出现转移性疾病的几率更高(OR 2.37;95%CI 2.11 - 2.66,<0.001)。在学术/研究机构治疗转移性黑色素瘤与社区癌症项目相比,死亡率更低(OR 0.75,95%CI 0.69 - 0.81,P值<0.001)。ICI引入后,白种人转移性黑色素瘤的生存率有所提高(调整后HR 0.80,95%CI 于0.78 - 0.83,<0.001);然而,这在AA患者(调整后HR 0.80,95%CI 0.62 - 1.02,P值 = 0.073)或眼部病例(HR 1.03,95%CI 0.81 - 1.31,P值 = 0.797)中无统计学意义。实际数据表明,自ICI引入以来,转移性黑色素瘤的生存率提高了20%。黑色素瘤AA患者初诊时转移性疾病几率过高,这表明需要更好地了解该疾病并改善医疗服务。