Department of Emergency Medicine, Yale School of Medicine, New Haven, Connecticut, USA.
MedStar Health National Center for Human Factors in Healthcare, Washington, DC, USA.
J Am Med Inform Assoc. 2021 Jul 14;28(7):1383-1392. doi: 10.1093/jamia/ocab011.
To derive 7 proposed core electronic health record (EHR) use metrics across 2 healthcare systems with different EHR vendor product installations and examine factors associated with EHR time.
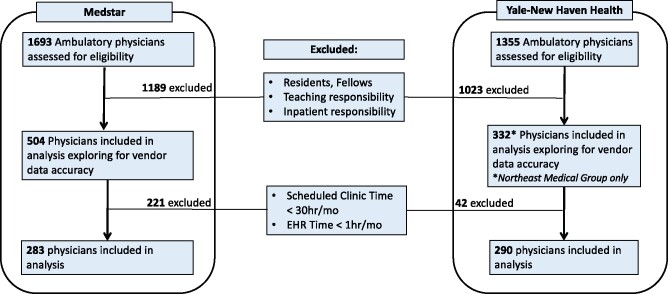
A cross-sectional analysis of ambulatory physicians EHR use across the Yale-New Haven and MedStar Health systems was performed for August 2019 using 7 proposed core EHR use metrics normalized to 8 hours of patient scheduled time.
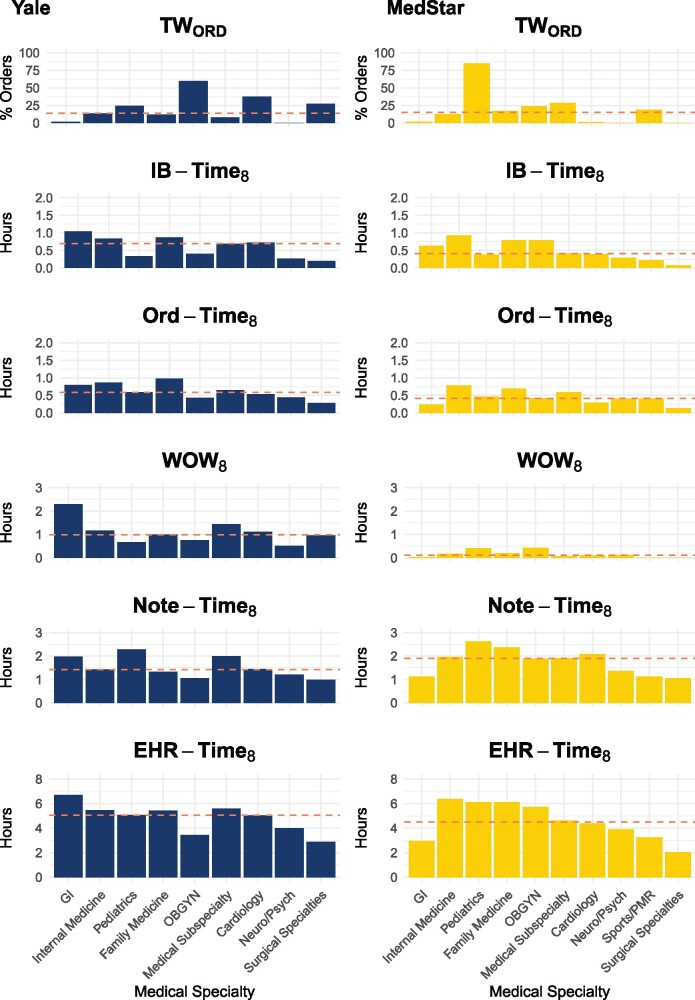
Five out of 7 proposed metrics could be measured in a population of nonteaching, exclusively ambulatory physicians. Among 573 physicians (Yale-New Haven N = 290, MedStar N = 283) in the analysis, median EHR-Time8 was 5.23 hours. Gender, additional clinical hours scheduled, and certain medical specialties were associated with EHR-Time8 after adjusting for age and health system on multivariable analysis. For every 8 hours of scheduled patient time, the model predicted these differences in EHR time (P < .001, unless otherwise indicated): female physicians +0.58 hours; each additional clinical hour scheduled per month -0.01 hours; practicing cardiology -1.30 hours; medical subspecialties -0.89 hours (except gastroenterology, P = .002); neurology/psychiatry -2.60 hours; obstetrics/gynecology -1.88 hours; pediatrics -1.05 hours (P = .001); sports/physical medicine and rehabilitation -3.25 hours; and surgical specialties -3.65 hours.
For every 8 hours of scheduled patient time, ambulatory physicians spend more than 5 hours on the EHR. Physician gender, specialty, and number of clinical hours practicing are associated with differences in EHR time. While audit logs remain a powerful tool for understanding physician EHR use, additional transparency, granularity, and standardization of vendor-derived EHR use data definitions are still necessary to standardize EHR use measurement.
针对使用不同电子病历(EHR)供应商产品的两个医疗系统,推导出 7 项 EHR 使用的核心建议指标,并分析与 EHR 使用时间相关的因素。
2019 年 8 月,通过 7 项 EHR 使用的核心建议指标(将患者预约时间标准化为 8 小时),对耶鲁-纽黑文医疗系统(Yale-New Haven)和医疗之星健康系统(MedStar Health)的门诊医生 EHR 使用情况进行了横断面分析。
7 项建议指标中的 5 项可用于非教学型、仅限门诊的医生人群。在分析的 573 名医生(耶鲁-纽黑文:290 名,医疗之星:283 名)中,EHR-Time8 的中位数为 5.23 小时。经多变量分析调整年龄和医疗系统后,性别、额外安排的临床时间以及某些医学专业与 EHR-Time8 相关。对于每 8 小时的预约患者时间,该模型预测 EHR 时间的差异(P<.001,除非另有说明):女医生增加 0.58 小时;每月额外安排的临床时间增加 0.01 小时;心脏病学专业减少 1.30 小时;医学亚专科减少 0.89 小时(除胃肠病学外,P=.002);神经病学/精神病学减少 2.60 小时;妇产科减少 1.88 小时;儿科减少 1.05 小时(P=.001);运动/物理医学与康复减少 3.25 小时;外科专业减少 3.65 小时。
对于每 8 小时的预约患者时间,门诊医生在 EHR 上花费的时间超过 5 小时。医生的性别、专业和临床实践时间的数量与 EHR 使用时间的差异相关。虽然审计日志仍然是了解医生 EHR 使用情况的有力工具,但仍然需要增加供应商生成的 EHR 使用数据定义的透明度、粒度和标准化,以实现 EHR 使用的标准化测量。