Department of Anesthesiology, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, China.
Department of Anesthesiology, Pidu District People's Hospital, 156# East Street, Pitong Town, Pidu District, Chengdu, Sichuan, 611730, People's Republic of China.
BMC Anesthesiol. 2021 Apr 6;21(1):107. doi: 10.1186/s12871-021-01317-6.
We assessed whether a postoperative bilateral, ultrasound-guided, posterior transversus abdominis plane (TAP) block could reduce 24 h rescue tramadol requirement compared with placebo in patients undergoing elective laparoscopic colorectal cancer surgery.
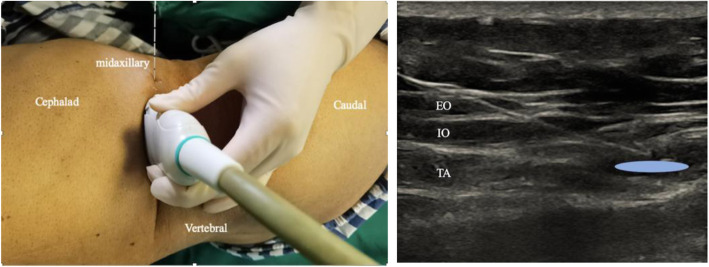
Patients scheduled to undergo elective laparoscopic surgery following the diagnosis of colorectal cancer were included in this study and randomized into Group and Group Control. The patients received a postoperative bilateral, ultrasound-guided, posterior TAP block in either 20 mL of 0.5% ropivacaine (Group TAP) per side or an equivalent volume of normal saline (Group Control). The primary outcome was the cumulative consumption of rescue tramadol within 24 h after the surgery. Secondary endpoints included (1) resting and movement numerical rating scale (NRS) pain scores at 2, 4, 6, 12, 24, 48, and 72 h; (2) incidences of related side effects; (3) time to the first request for rescue tramadol; (4) patient satisfaction regarding postoperative analgesia; (5) time to restoration of intestinal function; (6) time to mobilization; and (7) the length of hospital stay.
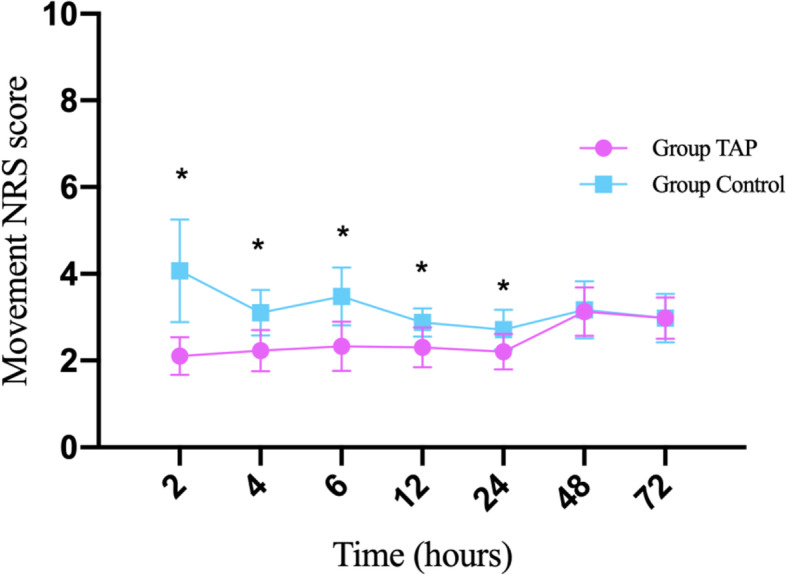
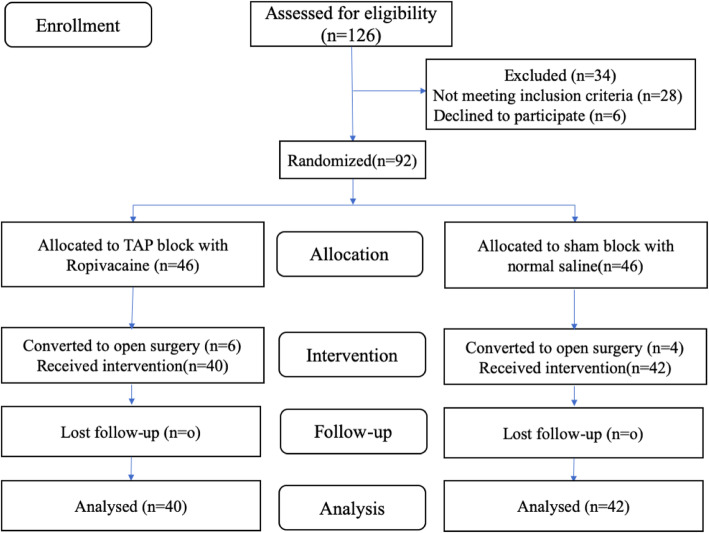
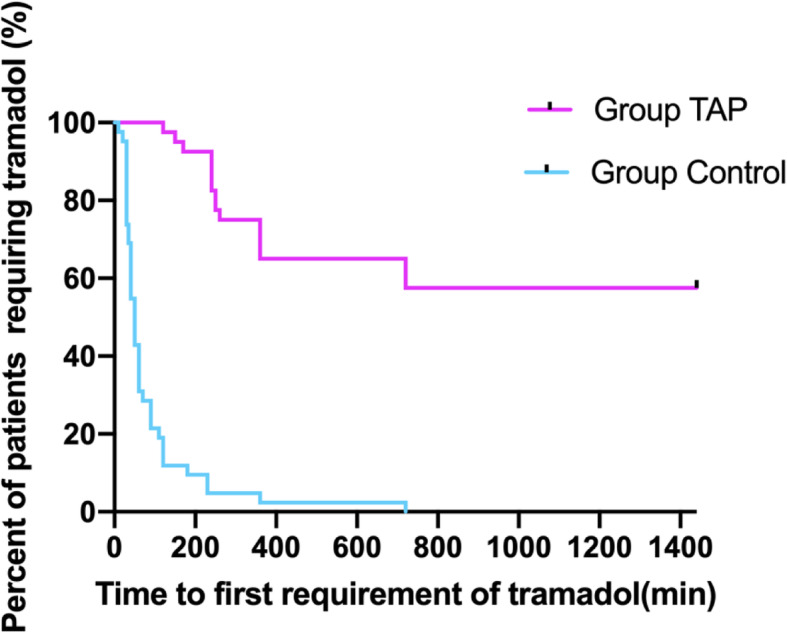
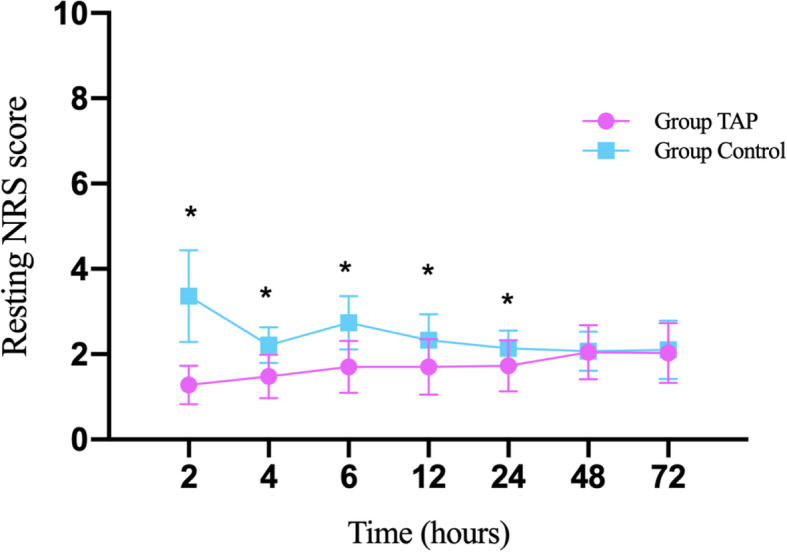
In total, 92 patients were randomized, and 82 patients completed the analysis. The total rescue tramadol requirement (median [interquartile range]) within the first 24 h was lower in Group TAP (0 [0, 87.5] mg) than in Group Control (100 [100, 200] mg), P < 0.001. The posterior TAP block reduced resting and movement NRS pain scores at 2, 4, 6, 12, and 24 h after surgery (all P < 0.001) but showed similar scores at 48 h or 72 h. A higher level of satisfaction with postoperative analgesia was observed in Group TAP on day 1 (P = 0.002), which was similar on days 2 (P = 0.702) and 3 (P = 0.551), compared with the Group Control. A few incidences of opioid-related side effects (P < 0.001) and a lower percentage of patients requiring rescue tramadol analgesia within 24 h (P < 0.001) were observed in Group TAP. The time to the first request for rescue analgesia was prolonged, and the time to mobilization and flatus was reduced with a shorter hospital stay in Group TAP as compared with Group Control.
A postoperative bilateral, ultrasound-guided, posterior TAP block resulted in better pain management and a faster recovery in patients undergoing laparoscopic colorectal cancer surgery, without adverse effects.
The study was registered at http://www.chictr.org.cn ( ChiCTR-IPR-17012650 ; Sep 12, 2017).
我们评估了在接受择期腹腔镜结直肠癌手术的患者中,与安慰剂相比,术后双侧、超声引导、腹横肌平面(TAP)阻滞是否可以减少 24 小时内曲马多的补救需求。
本研究纳入了诊断为结直肠癌后拟行择期腹腔镜手术的患者,并将其随机分为 TAP 组和对照组。术后,患者在每侧接受 20 毫升 0.5%罗哌卡因(TAP 组)或等量生理盐水(对照组)的双侧、超声引导、后路 TAP 阻滞。主要结局是术后 24 小时内曲马多的累积消耗量。次要终点包括(1)术后 2、4、6、12、24、48 和 72 小时静息和运动数字评分量表(NRS)疼痛评分;(2)相关不良反应发生率;(3)首次要求解救曲马多的时间;(4)患者对术后镇痛的满意度;(5)肠道功能恢复时间;(6)开始活动时间;(7)住院时间。
共纳入 92 例患者,82 例患者完成了分析。TAP 组(0[0,87.5]mg)术后 24 小时内曲马多总需求量(中位数[四分位数间距])明显低于对照组(100[100,200]mg),P<0.001。后路 TAP 阻滞可降低术后 2、4、6、12 和 24 小时的静息和运动 NRS 疼痛评分(均 P<0.001),但在 48 小时或 72 小时的评分相似。与对照组相比,TAP 组术后第 1 天(P=0.002)对术后镇痛的满意度更高,第 2 天(P=0.702)和第 3 天(P=0.551)相似。TAP 组发生阿片类药物相关不良反应的发生率较低(P<0.001),24 小时内需要曲马多解救镇痛的患者比例较低(P<0.001)。与对照组相比,TAP 组首次要求解救镇痛的时间延长,活动和排气时间缩短,住院时间缩短。
在接受腹腔镜结直肠癌手术的患者中,术后双侧、超声引导、后路 TAP 阻滞可更好地控制疼痛,促进患者快速康复,且无不良反应。
该研究在 http://www.chictr.org.cn(ChiCTR-IPR-17012650;2017 年 9 月 12 日)进行了注册。