Inam Fatima, Singh Priyanka R, Khalid Farhan, Javed Aqib, Shah Anuj R
Internal Medicine, King Edward Medical University, Lahore, PAK.
Internal Medicine, St Luke's Baylor Hospital, Houston, USA.
Cureus. 2021 Mar 3;13(3):e13675. doi: 10.7759/cureus.13675.
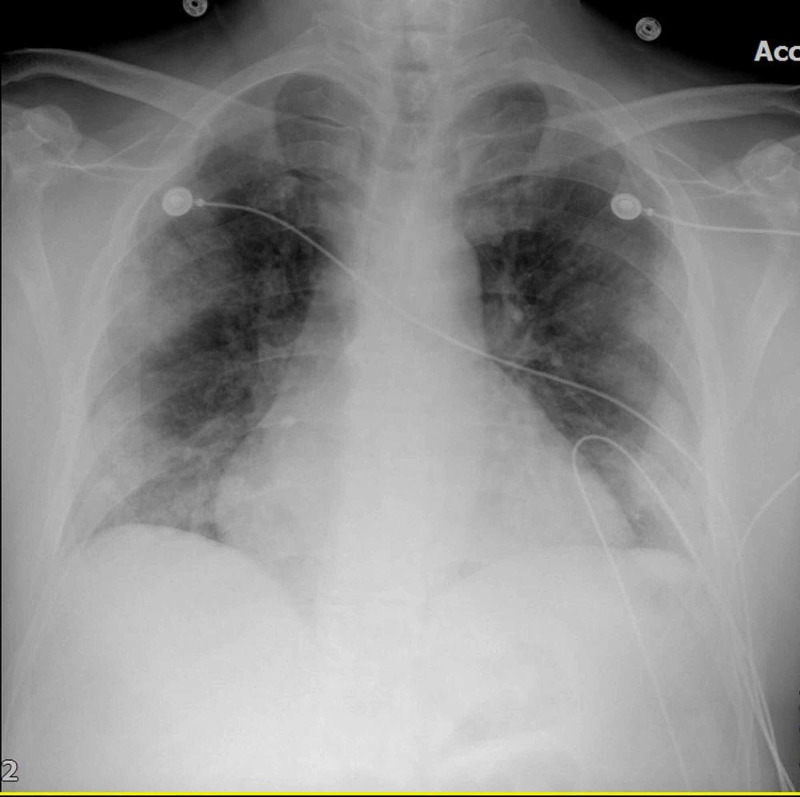
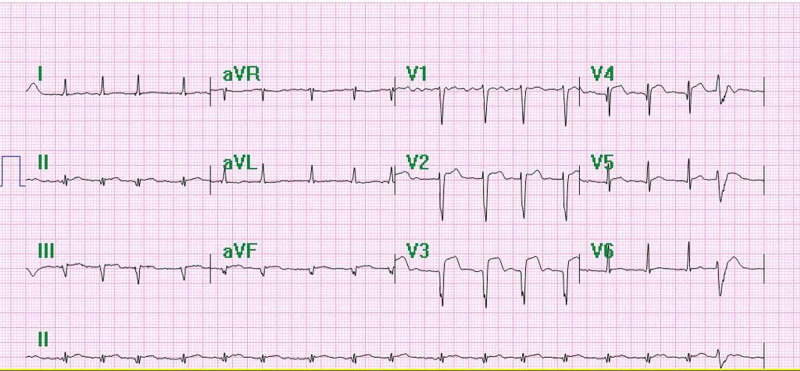
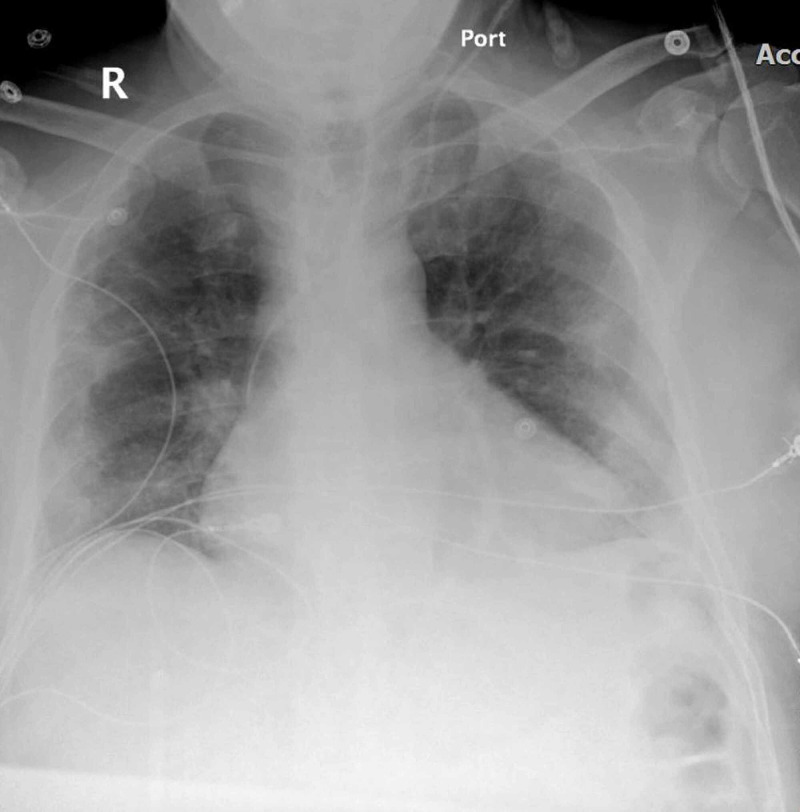
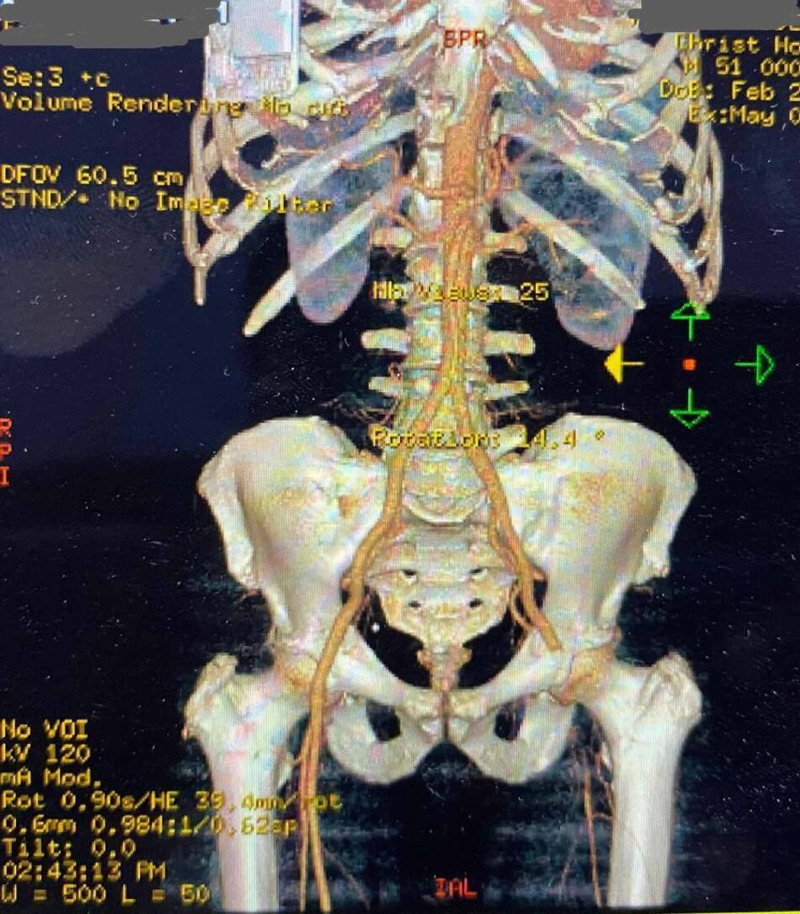
Novel coronavirus disease 2019 (COVID-19) is known to cause severe bilateral pneumonia and acute respiratory distress syndrome (ARDS), leading to difficulty breathing requiring mechanical ventilation and ICU management. In many patients, it has been found to cause severe hypercoagulability. We present a case of COVID-19 positive patient who developed myocardial infarction (MI) despite being on multiple anticoagulants. A 51-year-old, Middle-Eastern male diabetic patient presented to the emergency room with complaints of sudden onset left leg pain, paresthesias, and swelling for one day. On physical examination, the left leg was cool to touch from forefoot to mid-calf, with noticeable mottling over the forefoot and a nonpalpable dorsalis pedis. The patient was started on therapeutic enoxaparin and diltiazem in ED. Chest X-ray showed bilateral pulmonary infiltrates beginning peripherally and COVID-19 pneumonitis. The patient underwent a mechanical thrombectomy and was loaded with aspirin/clopidogrel, heparin drip, and enoxaparin. Despite being on triple anticoagulation, the patient had new-onset STEMI and elevated troponin levels. On angiography, the patient was found to have occluded mid-left anterior descending, most likely from acute on chronic thrombosis related to the patient's COVID-19 status. As flow could not be re-established, the patient was kept on long-term protective anticoagulation-triple therapy (an oral anticoagulant and dual antiplatelet therapy) and received pulmonary care for COVID-19 infection. The patient was discharged on long-term triple anticoagulation and COVID-19 precautions with scheduled retesting and follow-up.
新型冠状病毒肺炎2019(COVID-19)已知可导致严重的双侧肺炎和急性呼吸窘迫综合征(ARDS),导致呼吸困难,需要机械通气和重症监护病房管理。在许多患者中,已发现它会导致严重的高凝状态。我们报告一例COVID-19阳性患者,尽管使用了多种抗凝剂,仍发生了心肌梗死(MI)。一名51岁的中东男性糖尿病患者因突发左腿疼痛、感觉异常和肿胀一天而到急诊室就诊。体格检查发现,左腿从前足到小腿中部触之发凉,前足有明显的斑纹,足背动脉搏动未触及。患者在急诊室开始接受治疗剂量的依诺肝素和地尔硫䓬治疗。胸部X线显示双侧肺外周开始出现浸润及COVID-19肺炎。患者接受了机械取栓术,并给予阿司匹林/氯吡格雷负荷剂量、肝素滴注和依诺肝素治疗。尽管进行了三联抗凝治疗,患者仍出现了新发ST段抬高型心肌梗死(STEMI)且肌钙蛋白水平升高。血管造影显示,患者左前降支中段闭塞,最可能是与患者COVID-19状态相关的急性慢性血栓形成所致。由于血流无法重建,患者继续接受长期保护性抗凝三联治疗(一种口服抗凝剂和双重抗血小板治疗),并接受了针对COVID-19感染的肺部护理。患者出院时接受长期三联抗凝治疗并采取COVID-19预防措施,定期进行复查和随访。