Shawkat Ahmed, Merrell Eric T, Fadel Ghada A, Amzuta Ioana, Amin Hossam, Shah Amish J, Habeb Hanan, Aiash Hani
Department of Pulmonary Medicine and Critical Care, SUNY Upstate Medical University, Syracuse, NY, USA.
Department of Medicine, SUNY Upstate Medical University, Syracuse, NY, USA.
Am J Case Rep. 2020 Jul 22;21:e925786. doi: 10.12659/AJCR.925786.
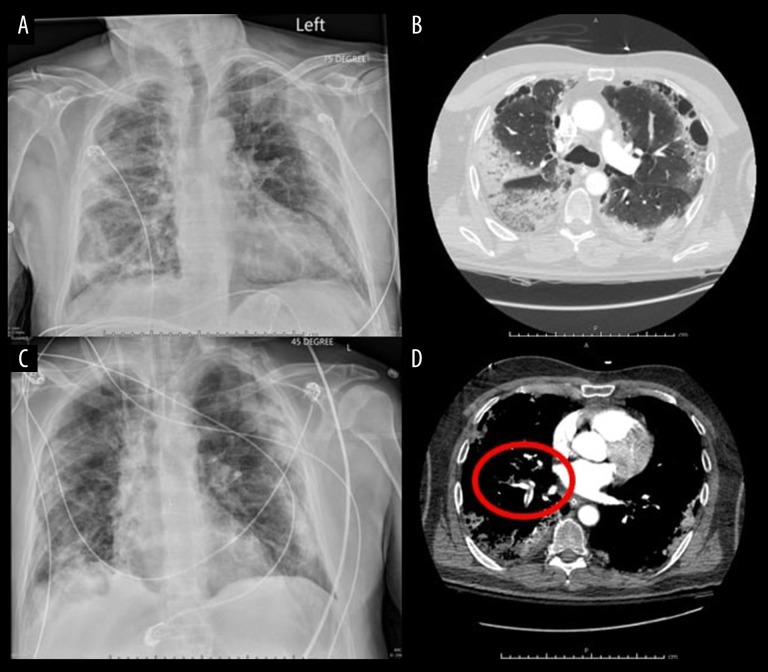
BACKGROUND Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the viral pathogen responsible for coronavirus disease 2019 (COVID-19), a pandemic respiratory illness. While many patients experience mild to moderate symptoms, severely affected patients often progress to acute respiratory distress syndrome (ARDS). Specific to COVID-19, abnormal coagulability appears to be a principal instigator in the progression of disease severity and mortality. In this report we summarize a case of COVID-19 in which extreme thrombophilia led to patient demise. CASE REPORT A 67-year-old man in New York presented to the hospital 14 days after testing positive for SARS-CoV-2 at an outpatient site. His initial presenting symptoms included sore throat, headache, fever, and diarrhea. He was brought in by his wife after developing sudden onset confusion and dysarthria. The patient's clinical picture, which was unstable on presentation, further deteriorated to involve significant desaturations, generalized seizure activity, and cardiac arrest requiring resuscitation. Upon return to spontaneous circulation, the patient required intensive care unit admission, mechanical ventilation, and vasopressor increases. Comprehensive workup uncovered coagulopathy with multiple thrombotic events involving the brain and lungs as well as radiographic evidence of severe lung disease. In the face of an unfavorable clinical picture, the family opted for comfort care measures. CONCLUSIONS In this case report on a 67-year-old-man with COVID-19, we present an account of extreme hypercoagulability that led to multiple thrombotic events eventually resulting in the man's demise. Abnormal coagulation 14 days from positive testing raises the question of whether outpatients with COVID-19 should be screened for hypercoagulability and treated with prophylactic anticoagulation/antiplatelet agents.
背景 严重急性呼吸综合征冠状病毒2(SARS-CoV-2)是导致2019冠状病毒病(COVID-19)这一全球性呼吸道疾病的病毒病原体。虽然许多患者症状较轻至中度,但重症患者往往会发展为急性呼吸窘迫综合征(ARDS)。COVID-19特有的异常凝血似乎是疾病严重程度进展和死亡率的主要诱因。在本报告中,我们总结了一例因极端血栓形成倾向导致患者死亡的COVID-19病例。病例报告一名67岁纽约男子在门诊SARS-CoV-2检测呈阳性14天后入院。他最初的症状包括喉咙痛、头痛、发热和腹泻。在出现突发意识模糊和构音障碍后,他被妻子送至医院。患者就诊时临床情况不稳定,进一步恶化,出现明显的血氧饱和度下降、全身性癫痫发作活动和需要复苏的心脏骤停。恢复自主循环后,患者需要入住重症监护病房、进行机械通气并增加血管升压药用量。全面检查发现存在凝血病,伴有涉及脑和肺的多处血栓形成事件以及严重肺部疾病的影像学证据。鉴于临床情况不佳,家属选择了舒适护理措施。结论 在这份关于一名67岁COVID-19男性患者的病例报告中,我们描述了导致多处血栓形成事件最终导致该男子死亡的极端高凝状态。阳性检测14天后出现的异常凝血引发了一个问题,即COVID-19门诊患者是否应筛查高凝状态并接受预防性抗凝/抗血小板药物治疗。