D'Amario Domenico, Cammarano Michela, Quarta Rossella, Casamassima Fabio, Restivo Attilio, Bianco Massimiliano, Palmieri Vincenzo, Zeppilli Paolo
Department of Cardiovascular Sciences, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Largo Agostino Gemelli, 8, 00168 Rome, Italy.
Sports Medicine Unit, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Largo Agostino Gemelli, 8, 00168 Rome, Italy.
Eur Heart J Case Rep. 2021 Mar 31;5(3):ytab109. doi: 10.1093/ehjcr/ytab109. eCollection 2021 Mar.
Myocardial bridge (MB) is the most common inborn coronary artery variant, in which a portion of myocardium overlies a major epicardial coronary artery segment. Myocardial bridge has been for long considered a benign condition, although it has been shown to cause effort-related ischaemia.
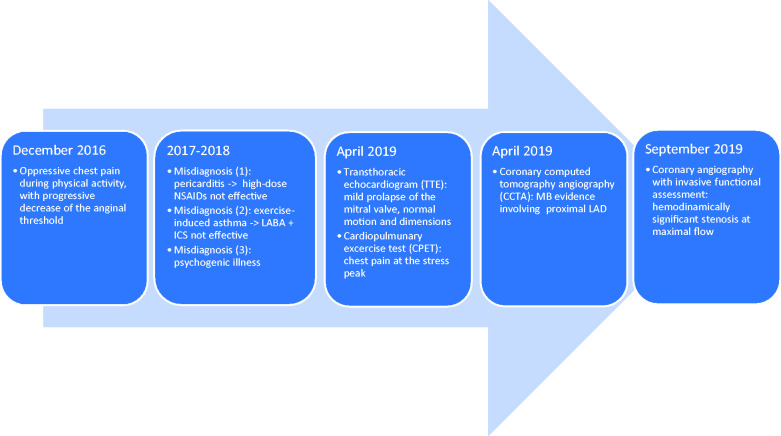
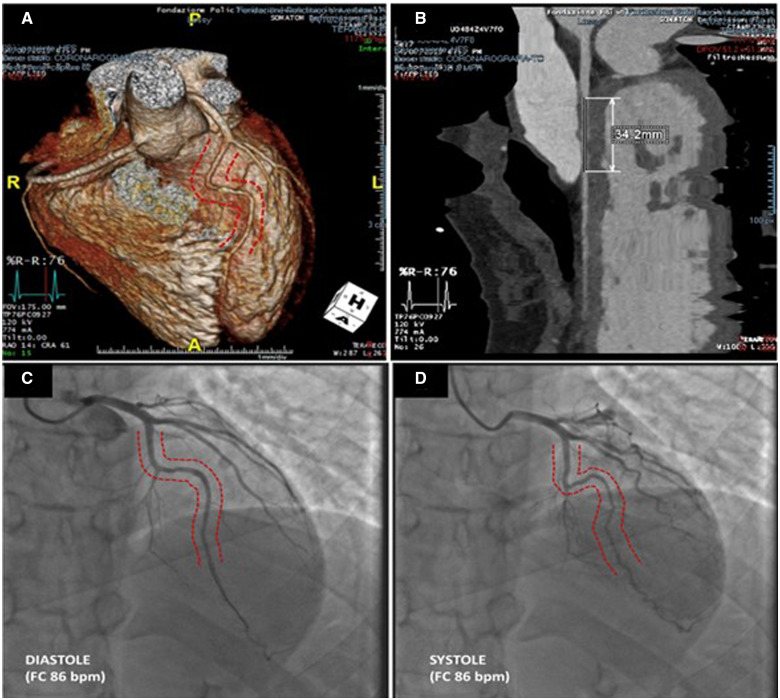
We present the case of a 17-year-old female patient experiencing chest pain during physical activity. Since her symptoms became unbearable, electrocardiogram and echocardiography were performed together with a coronary computed tomography scan, revealing an MB on proximal-mid left anterior descending artery. In order to unequivocally unmask the ischaemic burden lent by MB, the patient underwent coronary angiography and physiological invasive test: instantaneous wave-free ratio (iFR) and fractional flow reserve (FFR) were calculated, both at baseline and after dobutamine infusion (5 µg/kg/min). At baseline, iFR value was borderline (= 0.89), whereas after dobutamine infusion and increase in the heart rate, the patient suffered chest pain. This symptom was associated with a decrease in the iFR value up to 0.77. Consistently, when FFR was performed, a value of 0.92 was observed at baseline, while after inotrope infusion the FFR reached the haemodynamic significance (= 0.79). Therefore, a medical treatment with bisoprolol was started.
Our clinical case shows the importance of a comprehensive non-invasive and invasive assessment of MB in young patients experiencing chest pain, with significant limitation in the daily life. The coronary functional indexes allow to detect the presence of MB-derived ischaemia, thus guiding the decision to undertake a medical/surgical therapy.
心肌桥(MB)是最常见的先天性冠状动脉变异,其中一部分心肌覆盖主要的心外膜冠状动脉节段。尽管心肌桥已被证明会导致劳力性缺血,但长期以来一直被认为是一种良性疾病。
我们报告了一名17岁女性患者的病例,该患者在体力活动时出现胸痛。由于她的症状变得难以忍受,因此进行了心电图、超声心动图检查以及冠状动脉计算机断层扫描,结果显示左前降支近中段存在心肌桥。为了明确揭示心肌桥所致的缺血负担,该患者接受了冠状动脉造影和有创生理检查:计算了基线时以及多巴酚丁胺输注(5μg/kg/min)后的瞬间无波比值(iFR)和血流储备分数(FFR)。基线时,iFR值处于临界状态(=0.89),而在多巴酚丁胺输注和心率增加后,患者出现胸痛。该症状与iFR值降至0.77相关。同样,在进行FFR检查时,基线时观察到的值为0.92,而在输注正性肌力药物后,FFR达到血流动力学意义水平(=0.79)。因此,开始使用比索洛尔进行药物治疗。
我们的临床病例表明,对于有胸痛且日常生活受到严重限制的年轻患者,对心肌桥进行全面的非侵入性和侵入性评估非常重要。冠状动脉功能指标能够检测出心肌桥源性缺血的存在,从而指导采取药物/手术治疗的决策。