Department of Global Health, University of Washington Schools of Public Health and Medicine, Seattle.
Department of Civil and Environmental Engineering, University of Washington College of Engineering, Seattle.
JAMA Netw Open. 2021 Apr 1;4(4):e217373. doi: 10.1001/jamanetworkopen.2021.7373.
An accurate understanding of the distributional implications of public health policies is critical for ensuring equitable responses to the COVID-19 pandemic and future public health threats.
To identify and quantify the association of race/ethnicity-based, sex-based, and income-based inequities of state-specific lockdowns with 6 well-being dimensions in the United States.
DESIGN, SETTING, AND PARTICIPANTS: This pooled, repeated cross-sectional study used data from 14 187 762 households who participated in phase 1 of the population-representative US 2020 Household Pulse Survey (HPS). Households were invited to participate by email, text message, and/or telephone as many as 3 times. Data were collected via an online questionnaire from April 23 to July 21, 2020, and participants lived in all 50 US states and the District of Columbia.
Indicators of race/ethnicity, sex, and income and their intersections.
Unemployment; food insufficiency; mental health problems; no medical care received for health problems; default on last month's rent or mortgage; and class cancellations with no distance learning. Race/ethnicity, sex, income, and their intersections were used to measure distributional implications across historically marginalized populations; state-specific, time-varying population mobility was used to measure lockdown intensity. Logistic regression models with pooled repeated cross-sections were used to estimate risk of dichotomous outcomes by social group, adjusted for confounding variables.
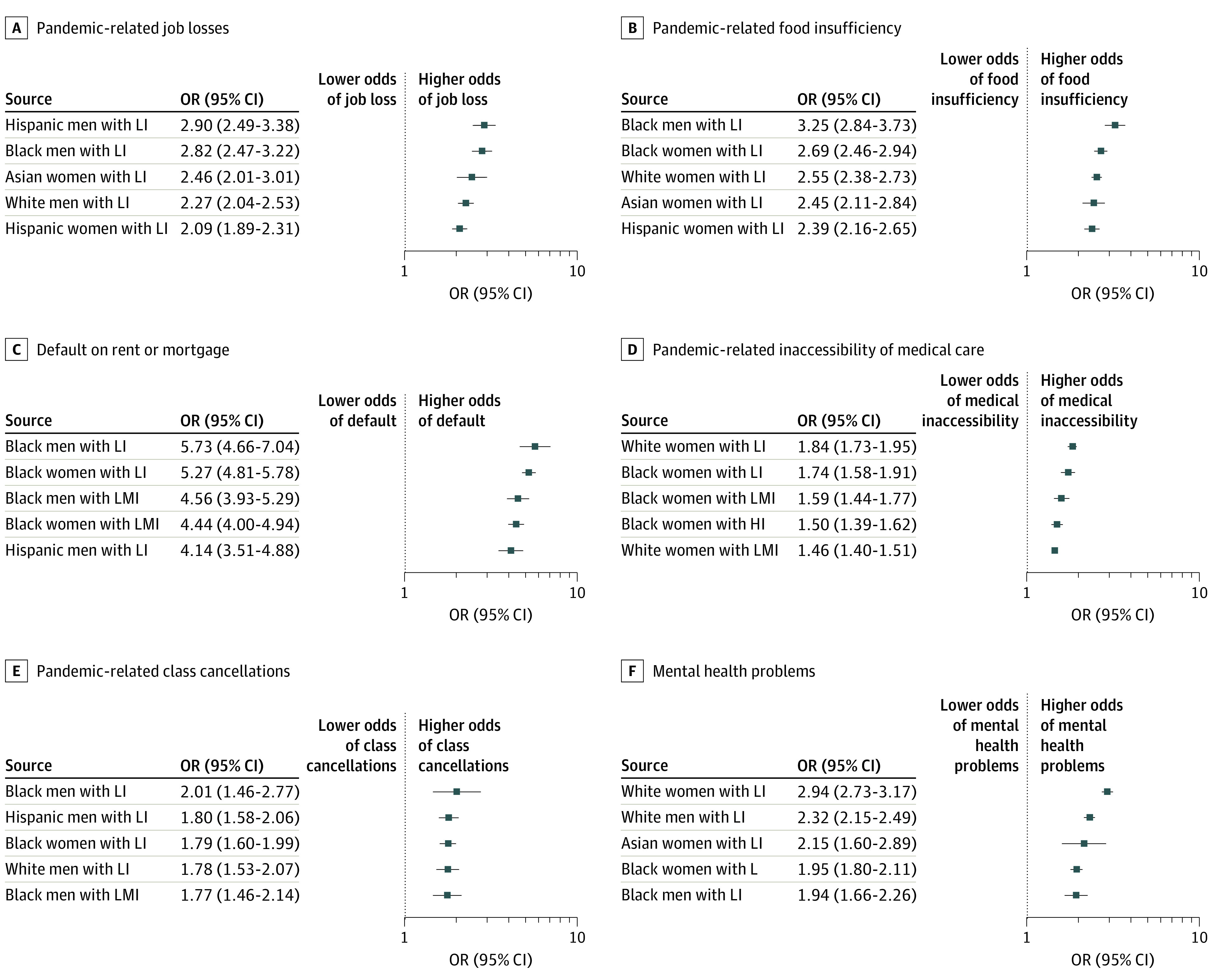
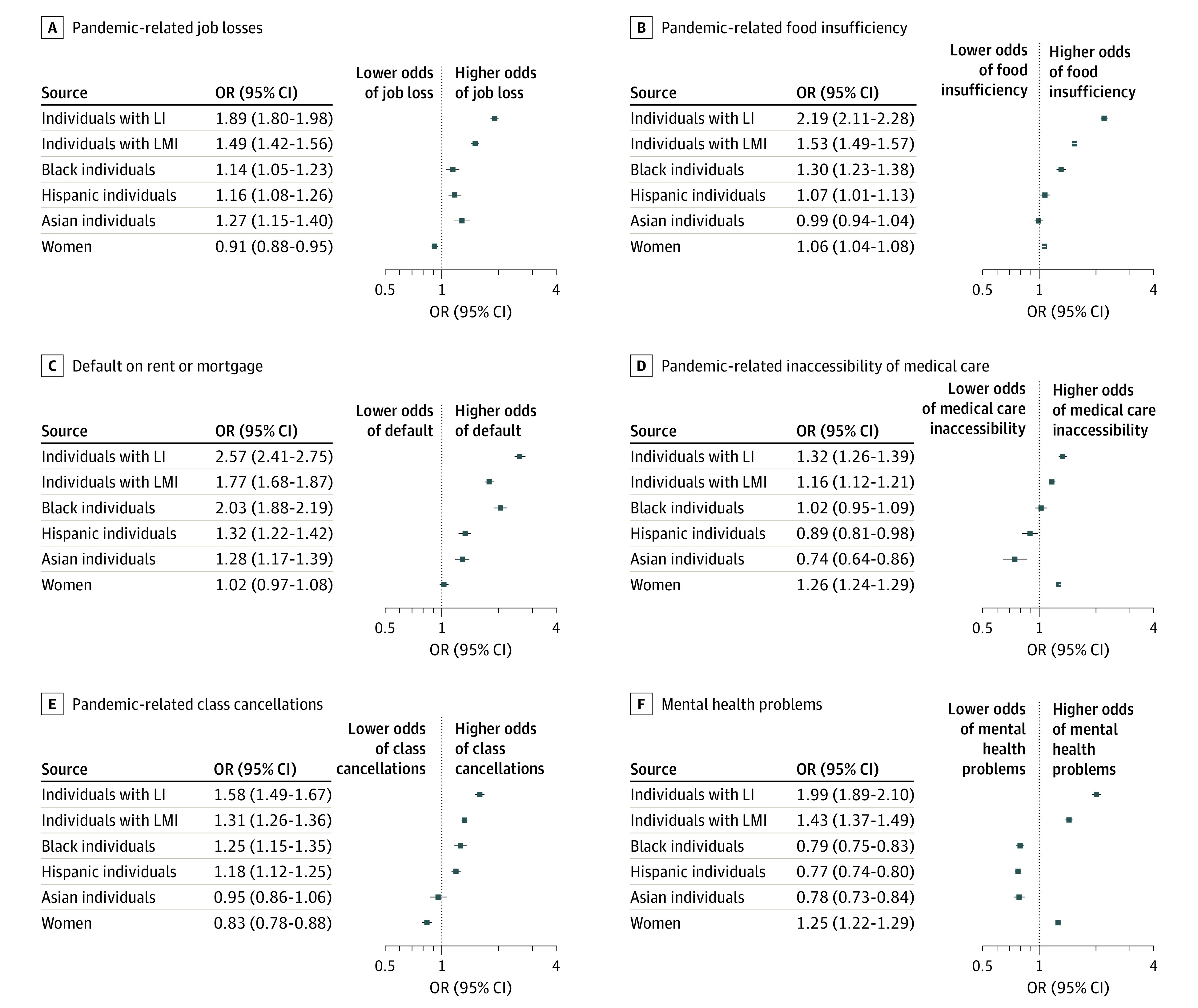
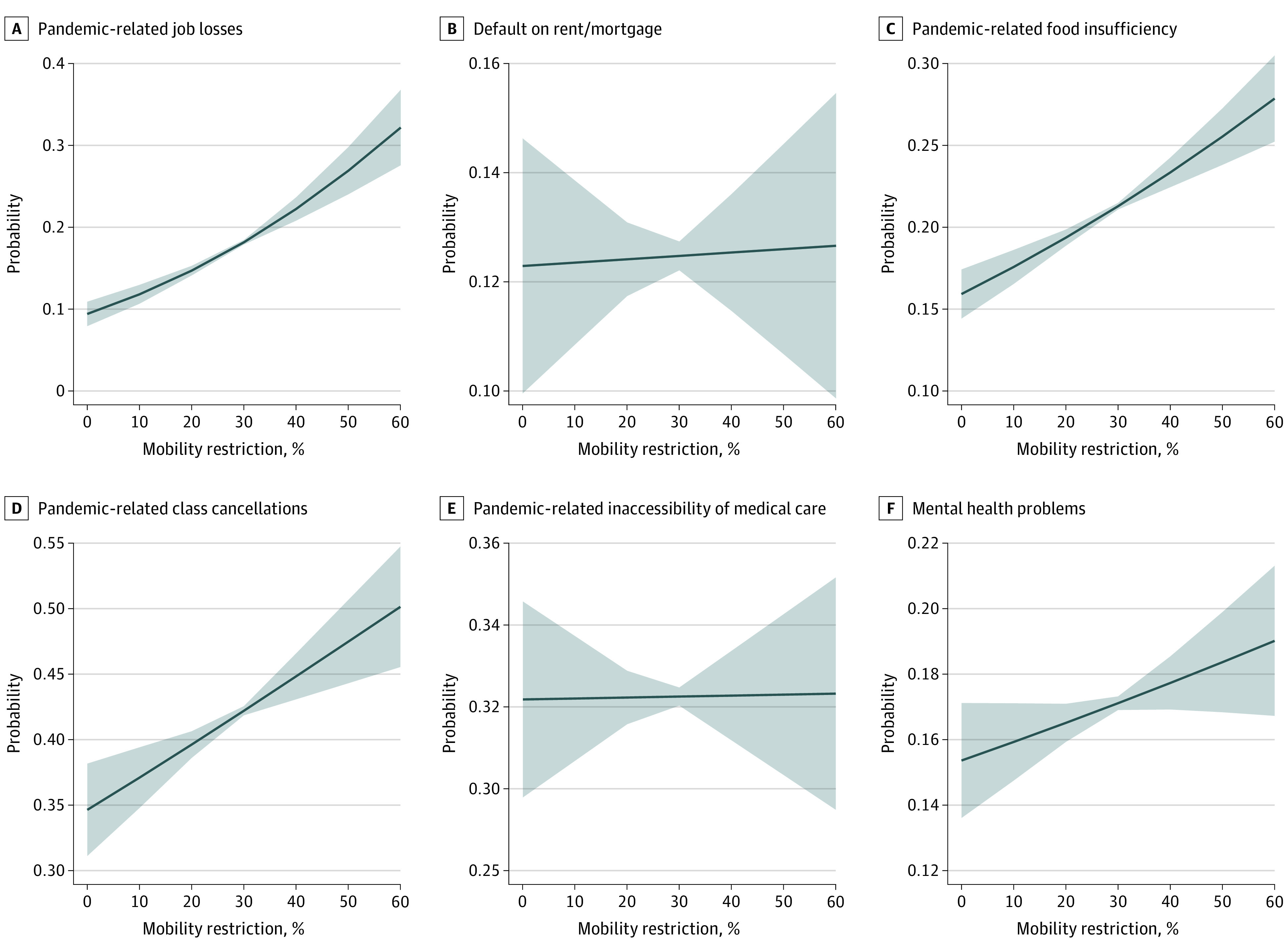
The 1 088 314 respondents (561 570 [51.6%; 95% CI, 51.4%-51.9%] women) were aged 18 to 88 years (mean [SD], 51.55 [15.74] years), and 826 039 (62.8%; 95% CI, 62.5%-63.1%) were non-Hispanic White individuals; 86 958 (12.5%; 95% CI, 12.4%-12.7%), African American individuals; 86 062 (15.2%; 95% CI, 15.0%-15.4%), Hispanic individuals; and 50 227 (5.6%; 95% CI, 5.5%-5.7%), Asian individuals. On average, every 10% reduction in mobility was associated with higher odds of unemployment (odds ratio [OR], 1.3; 95% CI, 1.2-1.4), food insufficiency (OR, 1.1; 95% CI, 1.1-1.2), mental health problems (OR, 1.04; 95% CI, 1.0-1.1), and class cancellations (OR, 1.1; 95% CI, 1.1-1.2). Across most dimensions compared with White men with high income, African American individuals with low income experienced the highest risks (eg, food insufficiency, men: OR, 3.3; 95% CI, 2.8-3.7; mental health problems, women: OR, 1.9; 95% CI, 1.8-2.1; medical care inaccessibility, women: OR, 1.7; 95% CI, 1.6-1.9; unemployment, men: OR, 2.8; 95% CI, 2.5-3.2; rent/mortgage defaults, men: OR, 5.7; 95% CI, 4.7-7.1). Other high-risk groups were Hispanic individuals (eg, unemployment, Hispanic men with low income: OR, 2.9; 95% CI, 2.5-3.4) and women with low income across all races/ethnicities (eg, medical care inaccessibility, non-Hispanic White women: OR, 1.8; 95% CI, 1.7-2.0).
In this cross-sectional study, African American and Hispanic individuals, women, and households with low income had higher odds of experiencing adverse outcomes associated with the COVID-19 pandemic and stay-at-home orders. Blanket public health policies ignoring existing distributions of risk to well-being may be associated with increased race/ethnicity-based, sex-based, and income-based inequities.
重要性:准确了解公共卫生政策的分布影响对于确保公平应对 COVID-19 大流行和未来的公共卫生威胁至关重要。
目的:确定和量化基于种族/族裔、性别和收入的不平等现象与美国 6 个福祉维度之间的关联,这些不平等现象与各州特定的封锁措施有关。
设计、设置和参与者:本研究采用了一项基于人群的重复横断面研究,使用了参加美国 2020 年家庭脉搏调查(HPS)第一阶段的 1476762 户家庭的数据。通过电子邮件、短信和/或电话多次邀请家庭参加。数据于 2020 年 4 月 23 日至 7 月 21 日通过在线问卷收集,参与者居住在美国所有 50 个州和哥伦比亚特区。
暴露:种族/族裔、性别和收入及其交叉指标。
主要结果和措施:失业;食品不足;心理健康问题;因健康问题未接受医疗护理;拖欠上月房租或抵押贷款;以及无远程学习的课程取消。种族/族裔、性别、收入及其交叉指标用于衡量历史上边缘化人群的分布影响;各州特定的、随时间变化的人口流动性用于衡量封锁强度。使用具有 pooled repeated cross-sections 的逻辑回归模型,根据混杂变量进行调整,估计社会群体的二分结果风险。
结果:1088314 名应答者(561570[51.6%;95%CI,51.4%-51.9%]名女性)年龄在 18 至 88 岁之间(平均[标准差],51.55[15.74]岁),826039 名(62.8%;95%CI,62.5%-63.1%)是非西班牙裔白人个体;86958 名(12.5%;95%CI,12.4%-12.7%)为非裔美国人个体;86062 名(15.2%;95%CI,15.0%-15.4%)为西班牙裔个体;50227 名(5.6%;95%CI,5.5%-5.7%)为亚裔个体。平均而言,每降低 10%的流动性与更高的失业风险相关(优势比[OR],1.3;95%CI,1.2-1.4)、食品不足(OR,1.1;95%CI,1.1-1.2)、心理健康问题(OR,1.04;95%CI,1.0-1.1)和课程取消(OR,1.1;95%CI,1.1-1.2)。与高收入的白人男性相比,在大多数维度上,非裔美国低收入个体的风险最高(例如,食品不足,男性:OR,3.3;95%CI,2.8-3.7;心理健康问题,女性:OR,1.9;95%CI,1.8-2.1;无法获得医疗保健,女性:OR,1.7;95%CI,1.6-1.9;失业,男性:OR,2.8;95%CI,2.5-3.2;拖欠租金/抵押贷款,男性:OR,5.7;95%CI,4.7-7.1)。其他高风险群体包括西班牙裔个体(例如,失业,低收入的西班牙裔男性:OR,2.9;95%CI,2.5-3.4)和所有种族/族裔的低收入女性(例如,无法获得医疗保健,非西班牙裔白人女性:OR,1.8;95%CI,1.7-2.0)。
结论和相关性:在这项横断面研究中,非裔美国人和西班牙裔个体、女性以及低收入家庭更有可能经历与 COVID-19 大流行和居家令相关的不良后果。忽视现有福祉风险分布的一刀切公共卫生政策可能与增加基于种族/族裔、性别和收入的不平等现象有关。