Obradovic Danilo, Rommel Karl-Philipp, Blazek Stephan, Klingel Karin, Gutberlet Matthias, Lücke Christian, Büttner Petra, Thiele Holger, Adams Volker, Lurz Philipp, Emrich Fabian, Besler Christian
Department of Internal Medicine/Cardiology, Heart Center Leipzig at the University of Leipzig and Leipzig Heart Institute, Strümpellstraße 39, Leipzig, 04289, Germany.
Cardiopathology, Institute for Pathology and Neuropathology, University Hospital Tübingen, Tübingen, Germany.
ESC Heart Fail. 2021 Jun;8(3):1850-1860. doi: 10.1002/ehf2.13304. Epub 2021 Apr 8.
Establishing a diagnosis of inflammatory cardiomyopathy (iCMP) by non-invasive means remains challenging despite advances in cardiac magnetic resonance imaging. Previous studies suggested the involvement of microRNAs in the pathogenesis of iCMP. We examined the association of a predefined set of circulatory microRNAs with clinical characteristics of iCMP and evaluated their diagnostic performance in suspected iCMP.
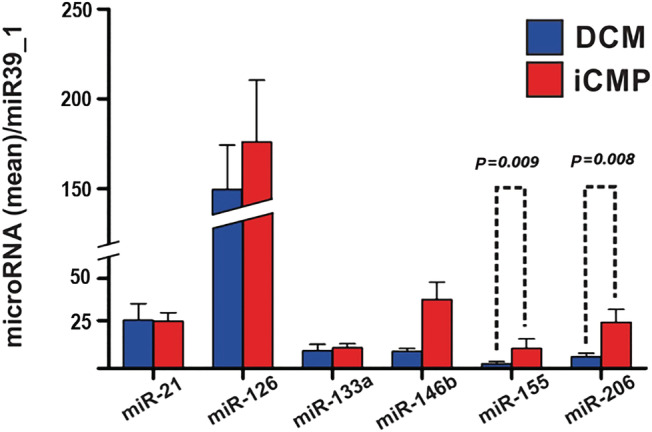
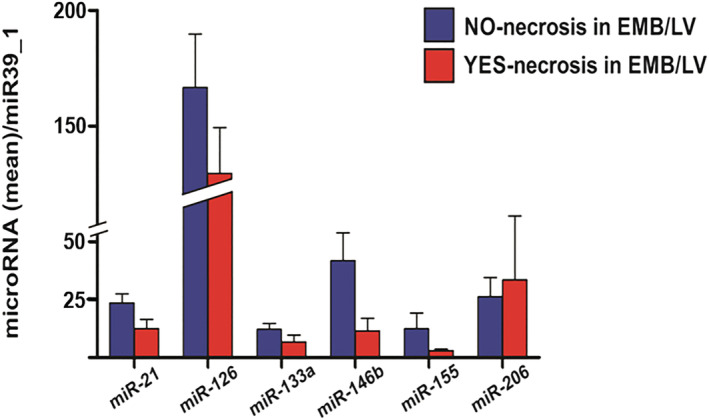
Eighty-nine patients with clinical suspicion of iCMP were included in the analysis. All patients underwent cardiac catheterization with left ventricular endomyocardial biopsy, echocardiography, and cardiac magnetic resonance imaging applying the Lake Louise criteria (LLC). Plasma levels of miR-21, miR-126, miR-133a, miR-146b, miR-155, and miR-206 were determined using real-time polymerase chain reaction. Based on immunohistological findings on endomyocardial biopsy, iCMP was diagnosed in 67% of study participants (n = 60). Plasma levels of miR-155 and miR-206 were significantly increased in patients with iCMP as compared with patients with dilated cardiomyopathy (P = 0.008 and P = 0.009, respectively). In receiver operating characteristic curve analysis, miR-155 and miR-206 demonstrated superior diagnostic performance for iCMP (0.68 and 0.67, respectively) compared with LLC [area under the curve (AUC) 0.60], Troponin T (AUC 0.51), and N-terminal pro-brain natriuretic peptide (AUC 0.51). While baseline miR-155 and miR-206 plasma levels were predictive for biopsy-proven iCMP (odds ratio = 2.61, 95% confidence interval = 1.28-5.31, P = 0.008 and odds ratio = 2.65, 95% confidence interval = 1.27-5.52, P = 0.009) on univariate logistic regression analysis, the presence of positive LLC, high baseline C-reactive protein, or presence of clinical symptoms and signs of viral infection failed to predict iCMP (P > 0.05, respectively).
The present data suggest that plasma levels of miR-206 and miR-155 are potential novel biomarkers for confirming the diagnosis of iCMP.
尽管心脏磁共振成像取得了进展,但通过非侵入性手段诊断炎症性心肌病(iCMP)仍然具有挑战性。先前的研究表明,微小RNA参与了iCMP的发病机制。我们研究了一组预先定义的循环微小RNA与iCMP临床特征的关联,并评估了它们在疑似iCMP中的诊断性能。
89例临床怀疑患有iCMP的患者纳入分析。所有患者均接受了心脏导管检查及左心室心内膜心肌活检、超声心动图检查,并采用路易斯湖标准(LLC)进行心脏磁共振成像检查。使用实时聚合酶链反应测定血浆中miR-21、miR-126、miR-133a、miR-146b、miR-155和miR-206的水平。根据心内膜心肌活检的免疫组织学结果,67%的研究参与者(n = 60)被诊断为iCMP。与扩张型心肌病患者相比,iCMP患者血浆中miR-155和miR-206的水平显著升高(分别为P = 0.008和P = 0.009)。在受试者工作特征曲线分析中,与LLC(曲线下面积[AUC]为0.60)、肌钙蛋白T(AUC为0.51)和N末端脑钠肽前体(AUC为0.51)相比,miR-155和miR-206对iCMP具有更好的诊断性能(分别为0.68和0.67)。在单因素逻辑回归分析中,基线miR-155和miR-206血浆水平可预测活检证实的iCMP(优势比分别为2.61,95%置信区间为1.28 - 5.31,P = 0.008;优势比为2.65,95%置信区间为1.27 - 5.52,P = 0.009),而LLC阳性、基线高C反应蛋白或存在病毒感染的临床症状和体征则无法预测iCMP(P均> 0.05)。
目前的数据表明,miR-206和miR-155的血浆水平是确认iCMP诊断的潜在新型生物标志物。