Department of Radiology, Chongqing Health Center for Women and Children, 120 Longshan Road, Chongqing, 400021, China.
Department of Radiology, Xiaochang First People's Hospital, 1 Station Front Road, Xiaochang, 432900, Hubei, China.
Sci Rep. 2021 Apr 8;11(1):7752. doi: 10.1038/s41598-021-87430-5.
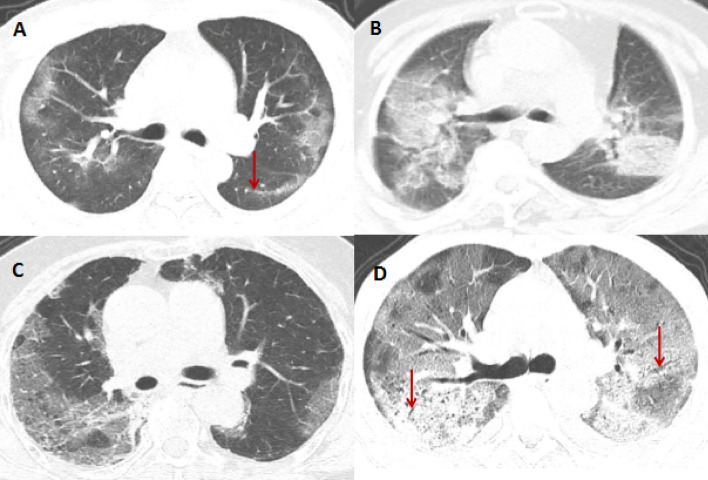
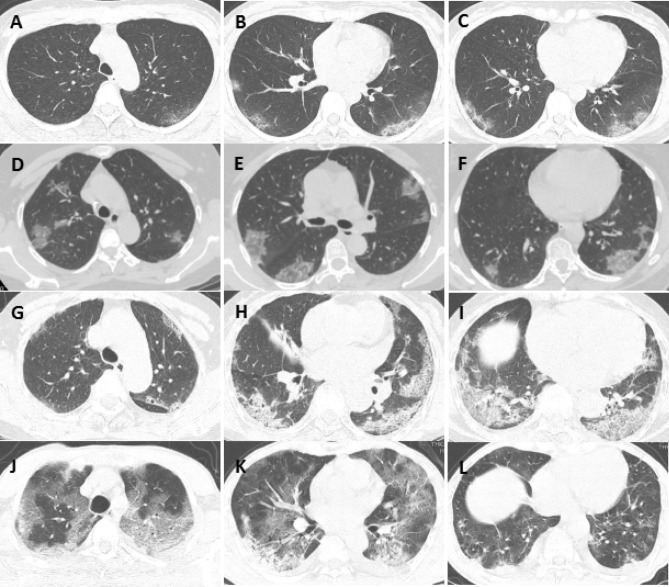
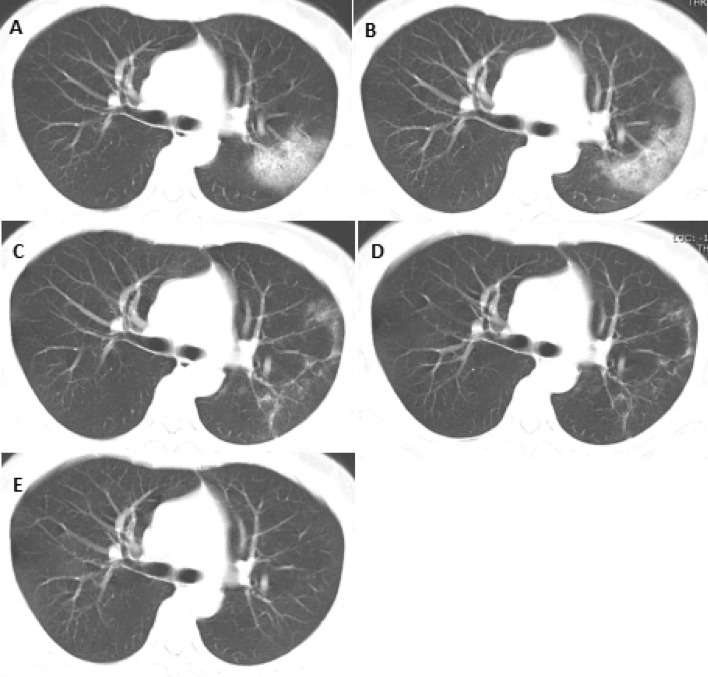
To explore the clinical application value of chest CT quantitative pulmonary inflammation index (PII) in the evaluation of the course and treatment outcome of COVID-19 pneumonia. One hundred and eighteen patients with COVID-19 pneumonia diagnosed by RT-PCR were analyzed retrospectively. The correlation between chest CT PII, clinical symptoms and laboratory examinations during the entire hospitalization period was compared. The average age of the patients was 46.0 ± 15 (range: 1-74) years. Of the 118 patients, 62 are male (52.5%) and 56 are female (47.5%). Among them, 116 patients recovered and were discharged, 2 patients died, and the median length of hospital stay was 22 (range: 9-41) days. On admission, 76.3% of the patients presented with fever, and the laboratory studies showed a decrease in lymphocyte (LYM) count and an increase in lactate dehydrogenase (LDH) levels, C-reactive protein (CRP) levels, and erythrocyte sedimentation rate (ESR). Within the studies' chest CTs, the median number of involved lung lobes was 4 (range: 0-5) and the median number of involved lung segments was 9 (range 0-20). The left lower lobe and the right lower lobe were the most likely areas to be involved (89.0% and 83.9%), and 84.7% of the patients had inflammatory changes in both lungs. The main manifestations on chest CT were ground glass opacities (31.4%), ground glass opacities and consolidation (20.3%), ground glass opacities and reticular patterns (32.2%), mixed type (13.6%), and white lungs (1.7%); common accompanying signs included linear opacities (55.9%), air bronchograms (46.6%), thick small vessel shadows (36.4%), and pleural hypertrophy (13.6%). The chest CT at discharge showed complete absorption of lesions in 19 cases (16.1%), but not in the remaining 99 cases. Lesions remained in a median of 3 lung lobes (range: 0-5). Residual lesions remained in a median of 5 lung segments (range: 0-20). The residual lesions mainly presented as ground glass opacities (61.0%), and the main accompanying sign was linear opacities (59.3%). Based on chest CT, the median maximum PII of lungs was 30.0% (range: 0-97.5%), and the median PII after discharge in the patients excluding the two deaths was 12.5% (range: 0-53.0%). PII was significantly negatively correlated with the LYM count and significantly positively correlated with body temperature, LDH, CRP, and ESR. There was no significant correlation between the PII and the white blood cell count, but the grade of PII correlated well with the clinical classification. PII can be used to monitor the severity and the treatment outcome of COVID-19 pneumonia, provide help for clinical classification, assist in treatment plan adjustments and aid assessments for discharge.
探讨胸部 CT 定量肺炎症指数(PII)在评估 COVID-19 肺炎病程和治疗效果中的临床应用价值。回顾性分析 118 例经 RT-PCR 诊断为 COVID-19 肺炎的患者。比较了整个住院期间胸部 CT PII 与临床症状和实验室检查的相关性。患者平均年龄为 46.0±15 岁(范围:1-74 岁)。118 例患者中,男性 62 例(52.5%),女性 56 例(47.5%)。其中 116 例痊愈出院,2 例死亡,中位住院时间为 22(范围:9-41)天。入院时,76.3%的患者发热,实验室检查显示淋巴细胞(LYM)计数减少,乳酸脱氢酶(LDH)、C 反应蛋白(CRP)和红细胞沉降率(ESR)水平升高。在研究中的胸部 CT 中,受累肺叶中位数为 4(范围:0-5),受累肺段中位数为 9(范围 0-20)。左下叶和右下叶是最有可能受累的部位(89.0%和 83.9%),84.7%的患者双肺均有炎症改变。胸部 CT 的主要表现为磨玻璃影(31.4%)、磨玻璃影伴实变(20.3%)、磨玻璃影伴网状影(32.2%)、混合类型(13.6%)和白肺(1.7%);常见伴随征象包括线状影(55.9%)、空气支气管征(46.6%)、小血管增厚影(36.4%)和胸膜肥厚(13.6%)。出院时胸部 CT 显示 19 例(16.1%)病变完全吸收,但其余 99 例未完全吸收。病变中位残留 3 个肺叶(范围:0-5)。病变中位残留 5 个肺段(范围:0-20)。残留病变主要表现为磨玻璃影(61.0%),主要伴随征象为线状影(59.3%)。根据胸部 CT,肺脏最大 PII 中位数为 30.0%(范围:0-97.5%),排除 2 例死亡患者后,出院时 PII 中位数为 12.5%(范围:0-53.0%)。PII 与 LYM 计数呈显著负相关,与体温、LDH、CRP 和 ESR 呈显著正相关。PII 与白细胞计数无显著相关性,但 PII 分级与临床分级相关性良好。PII 可用于监测 COVID-19 肺炎的严重程度和治疗效果,为临床分级提供帮助,协助治疗方案调整,并有助于评估出院。