Risch Lucie, Mayer Frank, Cassel Michael
University Outpatient Clinic, Sports Medicine and Orthopedics, University of Potsdam, Potsdam, Germany.
Faculty of Health Sciences, University of Potsdam, Potsdam, Germany.
Front Physiol. 2021 Mar 23;12:650507. doi: 10.3389/fphys.2021.650507. eCollection 2021.
The relationship between exercise-induced intratendinous blood flow (IBF) and tendon pathology or training exposure is unclear.
This study investigates the acute effect of running exercise on sonographic detectable IBF in healthy and tendinopathic Achilles tendons (ATs) of runners and recreational participants.
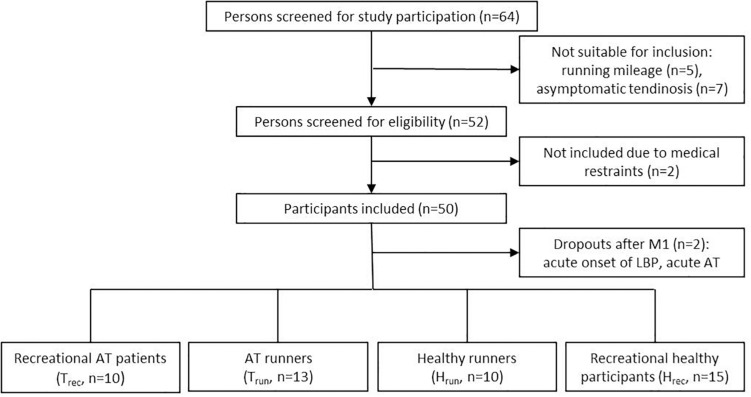
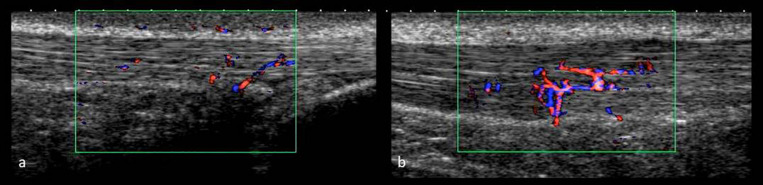
48 participants (43 ± 13 years, 176 ± 9 cm, 75 ± 11 kg) performed a standardized submaximal 30-min constant load treadmill run with Doppler ultrasound "Advanced dynamic flow" examinations before (U) and 5, 30, 60, and 120 min (U-U) afterward. Included were runners (>30 km/week) and recreational participants (<10 km/week) with healthy (H, = 10; H, = 15) or tendinopathic (T, = 13; T, = 10) ATs. IBF was assessed by counting number [n] of intratendinous vessels. IBF data are presented descriptively (%, median [minimum to maximum range] for baseline-IBF and IBF-difference post-exercise). Statistical differences for group and time point IBF and IBF changes were analyzed with Friedman and Kruskal-Wallis ANOVA (α = 0.05).
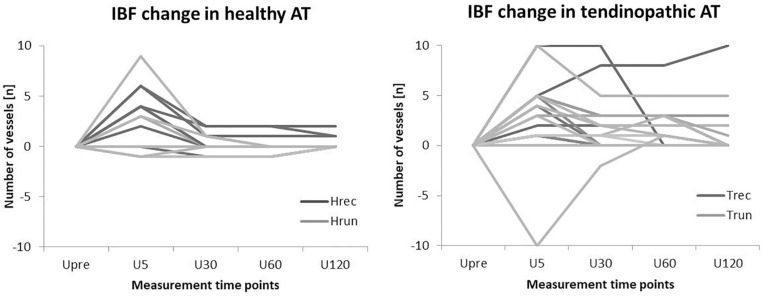
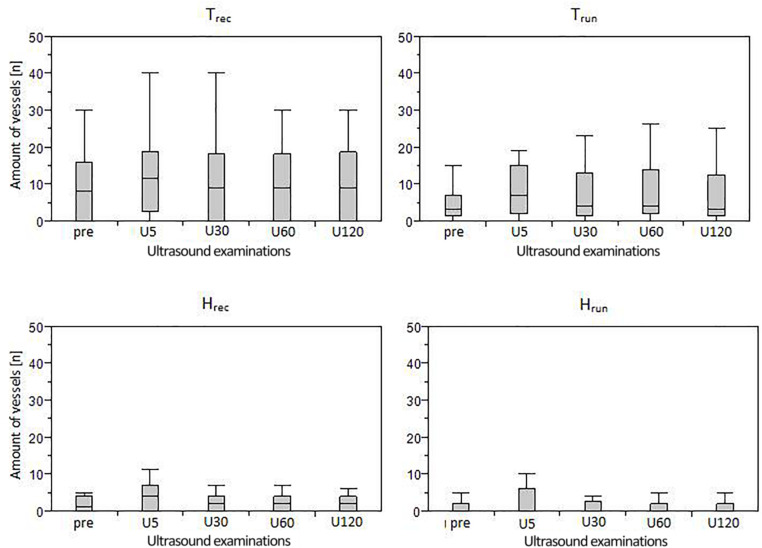
At baseline, IBF was detected in 40% (3 [1-6]) of H, in 53% (4 [1-5]) of H, in 85% (3 [1-25]) of T, and 70% (10 [2-30]) of T. At U IBF responded to exercise in 30% (3 [-1-9]) of H, in 53% (4 [-2-6]) of H, in 70% (4 [-10-10]) of T, and in 80% (5 [1-10]) of T. While IBF in 80% of healthy responding ATs returned to baseline at U, IBF remained elevated until U in 60% of tendinopathic ATs. Within groups, IBF changes from U-U were significant for H ( < 0.01), T ( = 0.05), and T ( < 0.01). Between groups, IBF changes in consecutive examinations were not significantly different ( > 0.05) but IBF-level was significantly higher at all measurement time points in tendinopathic versus healthy ATs ( < 0.05).
Irrespective of training status and tendon pathology, running leads to an immediate increase of IBF in responding tendons. This increase occurs shortly in healthy and prolonged in tendinopathic ATs. Training exposure does not alter IBF occurrence, but IBF level is elevated in tendon pathology. While an immediate exercise-induced IBF increase is a physiological response, prolonged IBF is considered a pathological finding associated with Achilles tendinopathy.
运动诱导的腱内血流(IBF)与肌腱病理或训练暴露之间的关系尚不清楚。
本研究调查跑步运动对跑步者和休闲参与者健康及患肌腱病的跟腱(AT)中超声可检测到的IBF的急性影响。
48名参与者(43±13岁,176±9厘米,75±11千克)进行了一次标准化的次最大强度30分钟恒定负荷跑步机跑步,在跑步前(U)以及跑步后5、30、60和120分钟(U-U)进行多普勒超声“高级动态血流”检查。纳入的有每周跑步超过30公里的跑步者和每周跑步少于10公里的休闲参与者,他们的跟腱健康(H,n = 10;H,n = 15)或患有肌腱病(T,n = 13;T,n = 10)。通过计算腱内血管数量[n]来评估IBF。IBF数据以描述性方式呈现(基线IBF和运动后IBF差异的百分比、中位数[最小至最大范围])。使用Friedman和Kruskal-Wallis方差分析(α = 0.05)分析组间和时间点的IBF及IBF变化的统计差异。
在基线时,H组中40%(3[1 - 6])、H组中53%(4[1 - 5])、T组中85%(3[1 - 25])以及T组中70%(10[2 - 30])检测到IBF。在U时,H组中30%(3[-1 - 9])、H组中53%(4[-2 - 6])、T组中70%(4[-10 - 10])以及T组中80%(5[1 - 10])的IBF对运动有反应。虽然80%有反应的健康跟腱中的IBF在U时恢复到基线,但60%患肌腱病的跟腱中的IBF在U时仍保持升高直至U。在组内,H组(P < 0.01)、T组(P = 0.05)和T组(P < 0.01)从U到U的IBF变化具有显著性。在组间,连续检查中的IBF变化无显著差异(P > 0.05),但在所有测量时间点,患肌腱病的跟腱与健康跟腱相比,IBF水平显著更高(P < 0.05)。
无论训练状态和肌腱病理情况如何,跑步都会导致有反应的肌腱中IBF立即增加。这种增加在健康跟腱中出现得很快,而在患肌腱病的跟腱中持续时间较长。训练暴露不会改变IBF的出现情况,但在肌腱病理状态下IBF水平会升高。虽然运动立即诱导的IBF增加是一种生理反应,但持续的IBF被认为是与跟腱病相关的病理表现。