Wu Wenxuan, Cheng Qiyang, Chen Junru, Chen Diyu, Feng Xiaode, Wu Jian
Division of Hepatobiliary and Pancreatic Surgery, Department of Surgery, First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, Zhejiang Province, China.
Key Laboratory of Combined Multi-organ Transplantation, Ministry of Public Health, First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, China.
World J Surg Oncol. 2021 Apr 10;19(1):107. doi: 10.1186/s12957-021-02213-6.
We aim to draw a conclusion which type of hepatectomy could be the priority for hilar cholangiocarcinoma patients.
Surgery is established as only potentially curative treatment for hilar cholangiocarcinoma. However, whether hepatectomy should be preferred to the left-side hepatectomy, which includes left hemihepatectomy, extended left hemihepatectomy, and left trisectionectomy, or right-side hepatectomy, which represents right hemihepatectomy, extended right hemihepatectomy, and right trisectionectomy, is debated. In this meta-analysis, we evaluated and compared the efficacy and safety of left-side hepatectomy and right-side hepatectomy in patients with hilar cholangiocarcinoma.
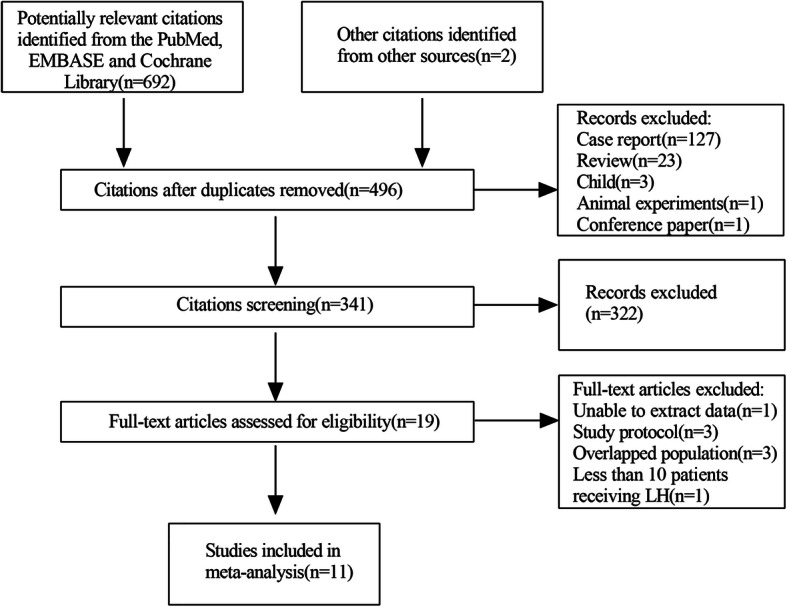
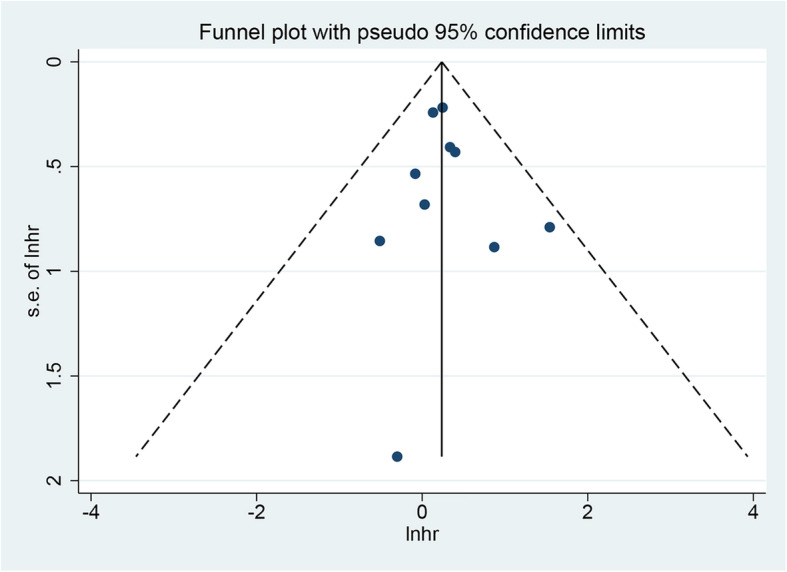
We systematically retrieved the MEDLINE, PubMed, and Cochrane library and related bibliography up to February 2020. The primary outcome is overall survival, and the secondary outcome includes 1-, 3-, and 5-year survival rates, morbidity, mortality, R0 resection rate, and operation time. Based on heterogeneity, fixed-effects model or random-effects models were established through meta-analysis.
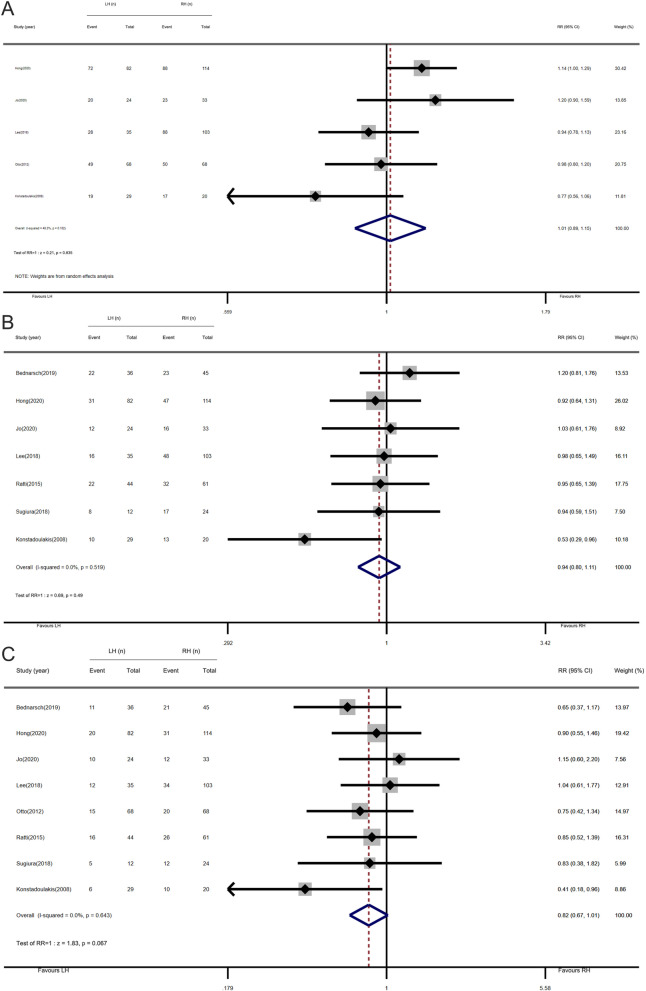
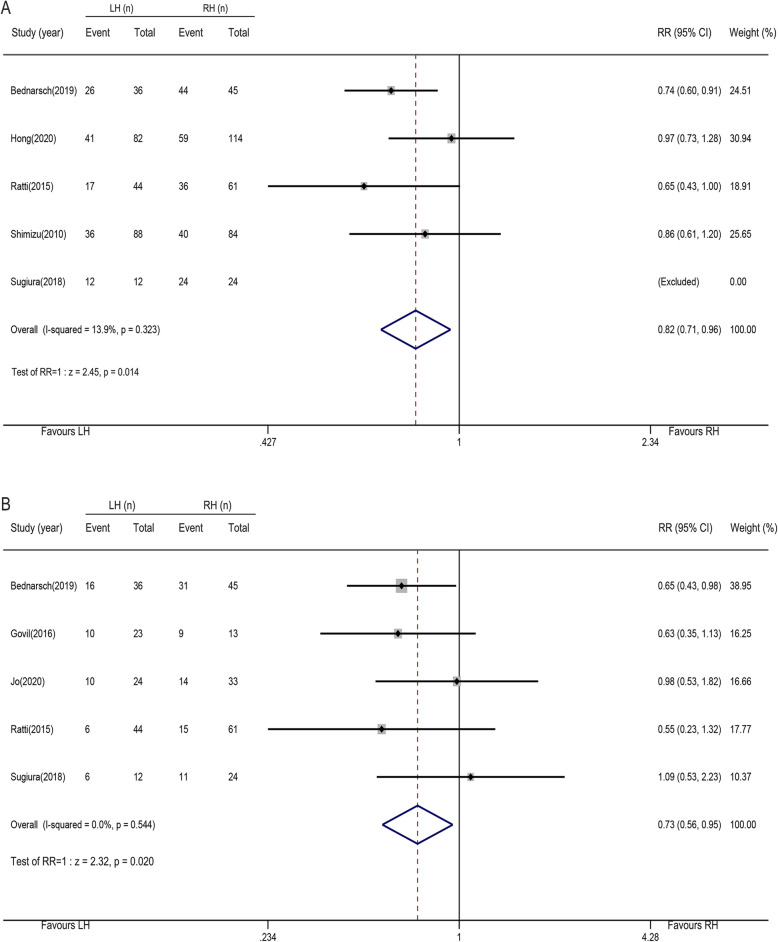
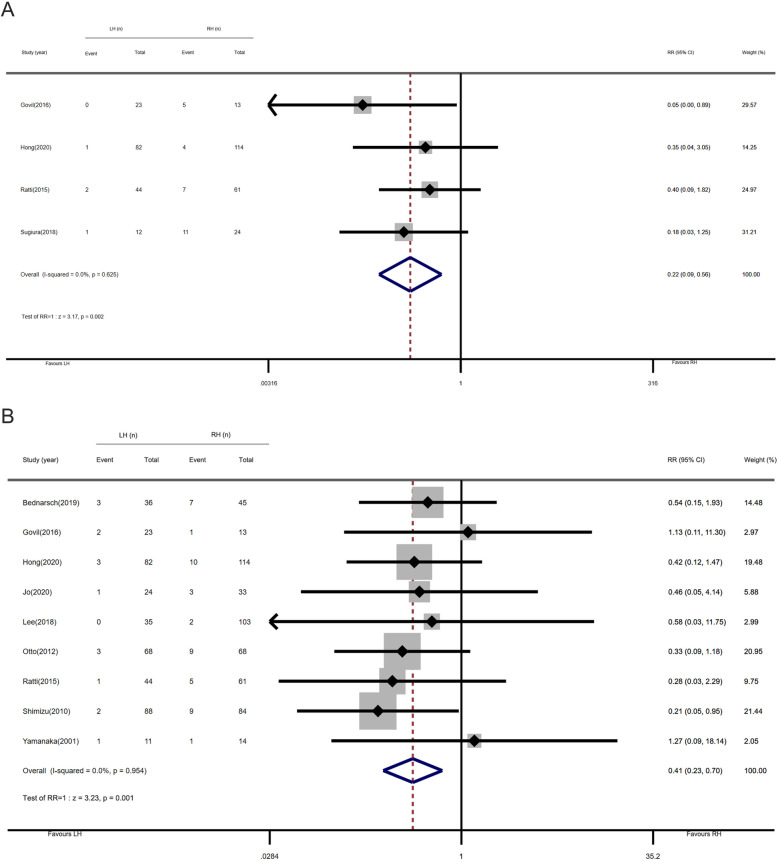
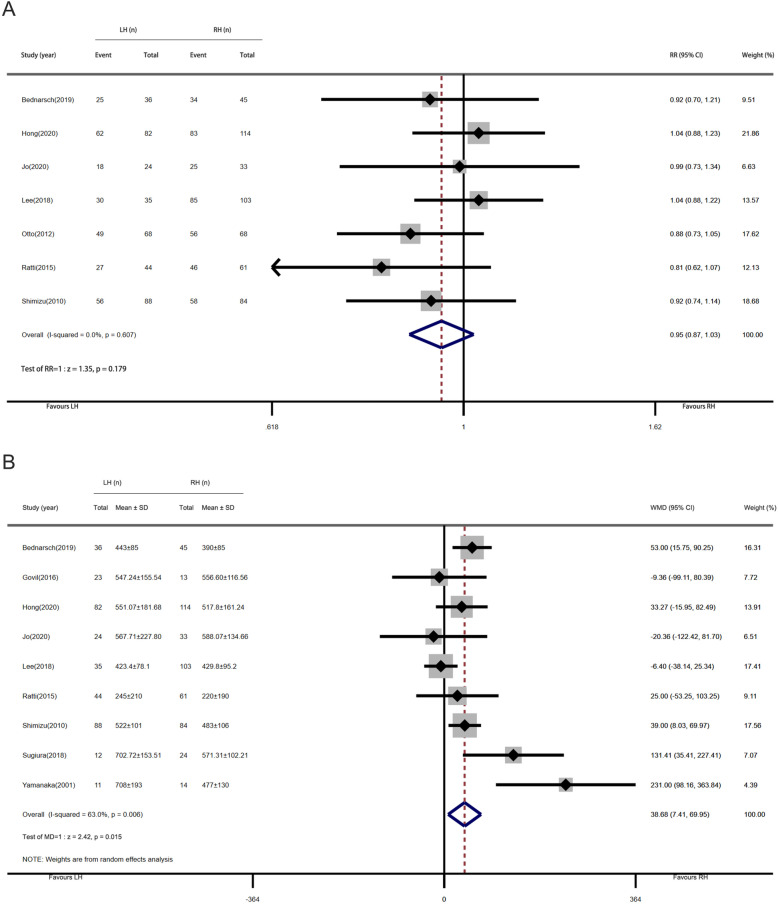
Eleven studies (11 cohort studies, totally 1031 patients) were involved in this study. The overall survival of patients who underwent left-side hepatectomy was comparable to that of patients who underwent right-side hepatectomy (hazard ratio, 1.27 [95% confidence interval, 0.98-1.63]). And there was no significant difference observed in 1-year (relative risk, 1.01 [95% CI, 0.89-1.15]), 3-year (relative risk, 0.94 [95% confidence interval, 0.80-1.11]), and 5-year survival (relative risk, 0.82 [95% confidence interval, 0.67-1.01]) rates between the left-side hepatectomy group and the right-side hepatectomy group. Comparing with the right-side hepatectomy cluster, the hilar cholangiocarcinoma patients in the left-side hepatectomy cluster presented better overall postoperative morbidity (relative risk, 0.82 [95% confidence interval, 0.71-0.96]) and major postoperative morbidity (relative risk, 0.73 [95% confidence interval, 0.56-0.95]). The post-hepatectomy liver failure rate (relative risk, 0.22 [95% confidence interval, 0.09-0.56]) and procedure-related mortality (relative risk, 0.41 [95% confidence interval, 0.23-0.70]) in the left-side hepatectomy group were better than those of the right-side hepatectomy group. Besides, the R0 resection rate was similar between the left-side hepatectomy group and the right-side hepatectomy group (relative risk, 0.95 [95% confidence interval, 0.87-1.03]). And the operation time for the left-side hepatectomy was significantly longer than that for the right-side hepatectomy (mean difference, 38.68 [95% confidence interval, 7.41-69.95]).
Through meta-analysis, we explored the comparable long-term outcomes and better short-term outcomes in the left-side hepatectomy group as is compared to the right-side hepatectomy group of hilar cholangiocarcinoma patients. In this study, the evidence obtained might indicate that the choice of left-side hepatectomy or right-side hepatectomy depends on the site of hilar cholangiocarcinoma in every patient.
我们旨在得出哪种肝切除术可作为肝门部胆管癌患者的首选术式。
手术是肝门部胆管癌唯一可能的治愈性治疗方法。然而,对于肝门部胆管癌患者,是选择左半肝切除术(包括左半肝切除术、扩大左半肝切除术和左三叶切除术)还是右半肝切除术(包括右半肝切除术、扩大右半肝切除术和右三叶切除术)更优,仍存在争议。在这项荟萃分析中,我们评估并比较了左半肝切除术和右半肝切除术治疗肝门部胆管癌患者的疗效和安全性。
我们系统检索了截至2020年2月的MEDLINE、PubMed和Cochrane图书馆以及相关参考文献。主要结局是总生存期,次要结局包括1年、3年和5年生存率、发病率、死亡率、R0切除率和手术时间。基于异质性,通过荟萃分析建立固定效应模型或随机效应模型。
本研究纳入了11项研究(11项队列研究,共1031例患者)。接受左半肝切除术患者的总生存期与接受右半肝切除术患者的总生存期相当(风险比,1.27[95%置信区间,0.98 - 1.63])。左半肝切除术组和右半肝切除术组在1年(相对风险,1.01[95%CI,0.89 - 1.15])、3年(相对风险,0.94[95%置信区间,0.80 - 1.11])和5年生存率(相对风险,0.82[95%置信区间,0.67 - 1.01])方面未观察到显著差异。与右半肝切除术组相比,左半肝切除术组的肝门部胆管癌患者术后总体发病率(相对风险,0.82[95%置信区间,0.71 - 0.96])和主要术后发病率(相对风险,0.73[95%置信区间,0.56 - 0.95])更低。左半肝切除术组的肝切除术后肝衰竭发生率(相对风险,0.22[95%置信区间,0.09 - 0.56])和手术相关死亡率(相对风险,0.41[95%置信区间,0.23 - 0.70])均低于右半肝切除术组。此外,左半肝切除术组和右半肝切除术组的R0切除率相似(相对风险,0.95[95%置信区间,0.87 - 1.03])。且左半肝切除术的手术时间显著长于右半肝切除术(平均差值,38.68[95%置信区间,7.41 - 69.95])。
通过荟萃分析,我们发现与肝门部胆管癌患者的右半肝切除术组相比,左半肝切除术组具有相当的长期结局和更好的短期结局。在本研究中,所获得的证据可能表明,左半肝切除术或右半肝切除术的选择应取决于每位患者肝门部胆管癌的位置。