Department of Liver Surgery, Liver Transplantation Division, West China Hospital, Sichuan University, Chengdu, 610041, China.
Laboratory of Liver Surgery, West China Hospital, Sichuan University, Chengdu, 610041, China.
World J Surg Oncol. 2021 Jul 20;19(1):218. doi: 10.1186/s12957-021-02330-2.
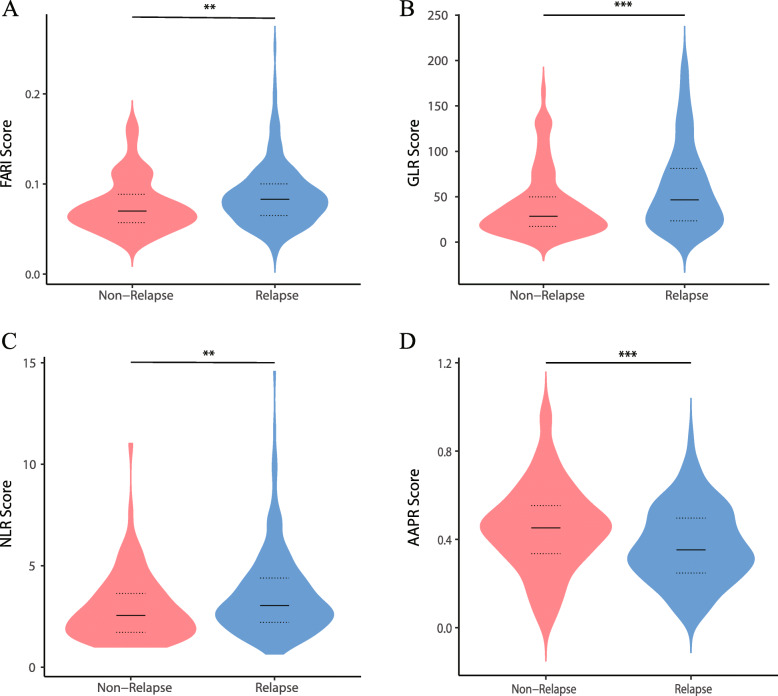
Systemic inflammation and nutritional status are associated with tumor development and progression. This study investigated the prognostic value of fibrinogen/albumin ratio index (FARI) in predicting recurrence-free survival (RFS) in patients with intrahepatic cholangiocarcinoma (ICC) undergoing hepatectomy.
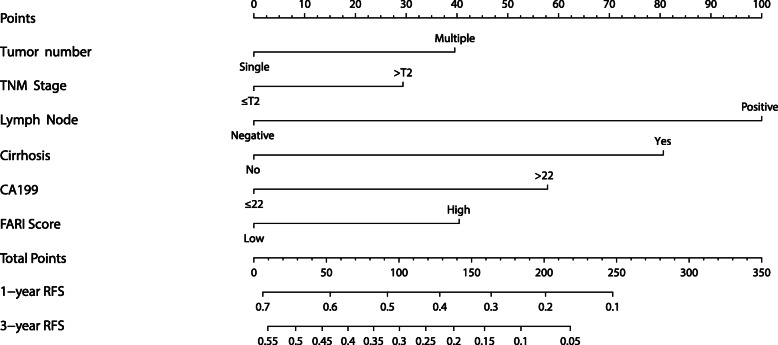
A retrospective cohort was conducted including patients who received curative hepatectomy for ICC at our hospital between May 2010 and December 2016. We collected the preoperative hematologic parameters and clinical data of all patients. Time-dependent receiver operating characteristic curve was used to identify the optimal cutoff value of FARI. The association between FARI-high and FARI-low group was investigated by using the Kaplan-Meier method. A nomogram based on the results of univariate and multivariate analysis was established.
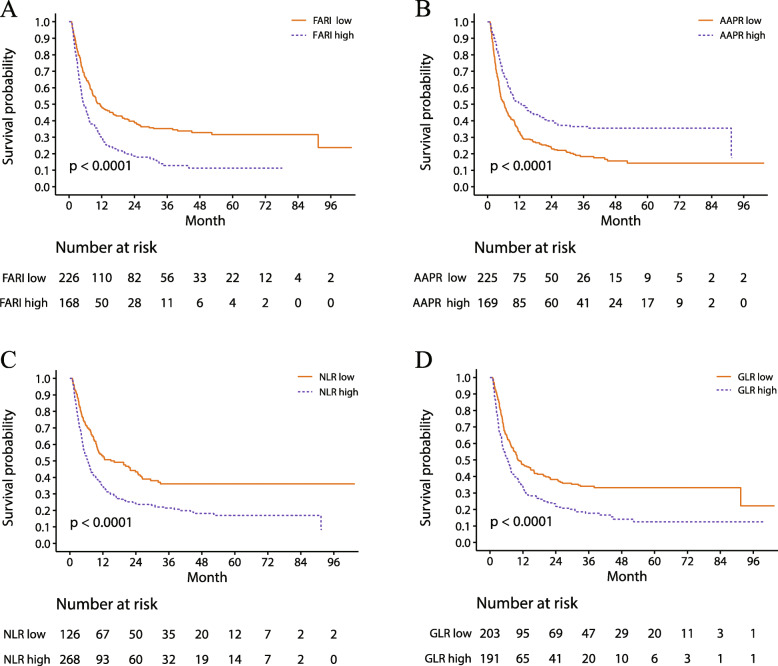
A total of 394 patients with ICC who underwent hepatectomy at our hospital were enrolled. K-M analysis revealed that increased FARI was related to reduced RFS (P < 0.001). The multivariate analysis indicated that tumor number, tumor-node-metastasis stage, lymph node metastasis, cirrhosis, serum carbohydrate antigen 19-9, and FARI were independent predictors of RFS, and the ROC curve analysis showed that the optimal cutoff value for FARI was 0.084 based on the Youden index. The nomogram for FARI showed satisfactory accuracy in predicting RFS for ICC patients undergoing hepatectomy (C index = 0.663; AIC = 3081.07).
Preoperative FARI is an independent predictor of RFS in patients undergoing hepatectomy for ICC, and the nomogram can be useful for clinical decision-making in the postoperative management of these patients.
全身性炎症和营养状况与肿瘤的发生和发展有关。本研究探讨了纤维蛋白原/白蛋白比值指数(FARI)在预测接受肝切除术的肝内胆管癌(ICC)患者无复发生存(RFS)中的预后价值。
本研究进行了一项回顾性队列研究,纳入了 2010 年 5 月至 2016 年 12 月期间在我院接受根治性肝切除术的 ICC 患者。我们收集了所有患者的术前血液学参数和临床数据。时间依赖性受试者工作特征曲线用于确定 FARI 的最佳截断值。Kaplan-Meier 法分析 FARI 高组和 FARI 低组之间的关系。基于单因素和多因素分析的结果建立了列线图。
共纳入了 394 例在我院接受肝切除术的 ICC 患者。K-M 分析显示,FARI 升高与 RFS 降低相关(P<0.001)。多因素分析表明,肿瘤数量、肿瘤-淋巴结-转移分期、淋巴结转移、肝硬化、血清碳水化合物抗原 19-9 和 FARI 是 RFS 的独立预测因素,ROC 曲线分析显示,基于 Youden 指数,FARI 的最佳截断值为 0.084。FARI 的列线图在预测 ICC 患者接受肝切除术后的 RFS 方面具有较好的准确性(C 指数=0.663;AIC=3081.07)。
术前 FARI 是 ICC 患者接受肝切除术 RFS 的独立预测因素,列线图可用于这些患者术后管理的临床决策。