Immunology Laboratory, Hôpital E. Herriot - Hospices Civils de Lyon, 5 place d'Arsonval, 69437, Lyon Cedex 03, France.
Joint Research Unit HCL-bioMérieux, EA 7426 "Pathophysiology of Injury-Induced Immunosuppression" (Université Claude Bernard Lyon 1 - Hospices Civils de Lyon - bioMérieux), 69003, Lyon, France.
Crit Care. 2021 Apr 12;25(1):140. doi: 10.1186/s13054-021-03558-w.
Since the onset of the pandemic, only few studies focused on longitudinal immune monitoring in critically ill COVID-19 patients with acute respiratory distress syndrome (ARDS) whereas their hospital stay may last for several weeks. Consequently, the question of whether immune parameters may drive or associate with delayed unfavorable outcome in these critically ill patients remains unsolved.
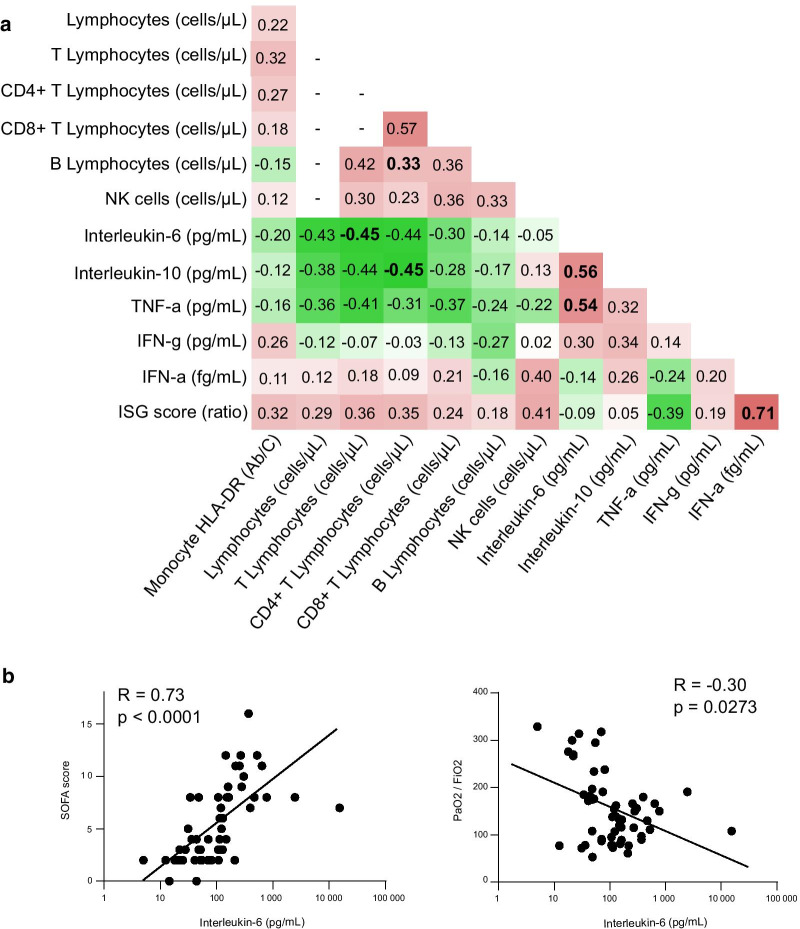
We present a dynamic description of immuno-inflammatory derangements in 64 critically ill COVID-19 patients including plasma IFNα2 levels and IFN-stimulated genes (ISG) score measurements.
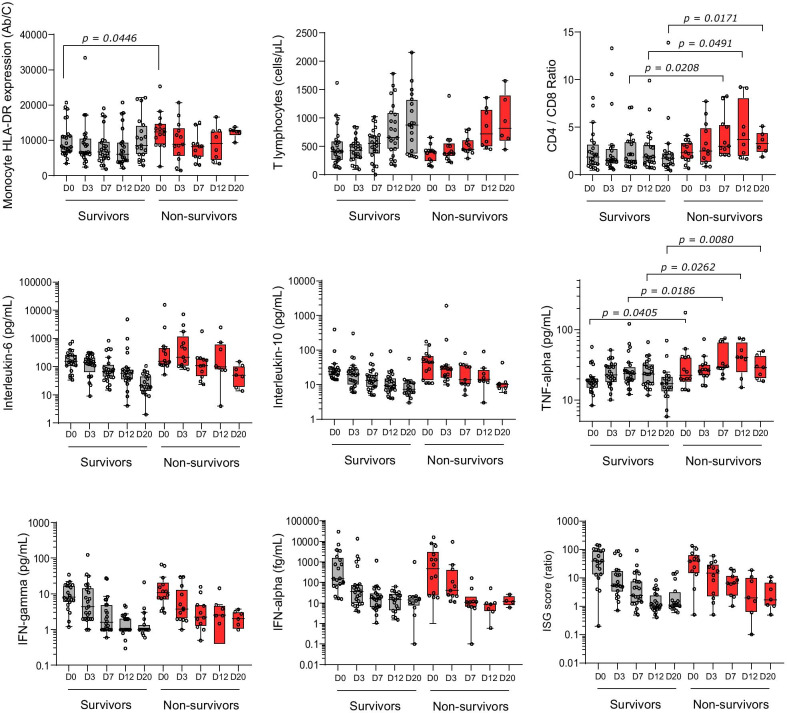
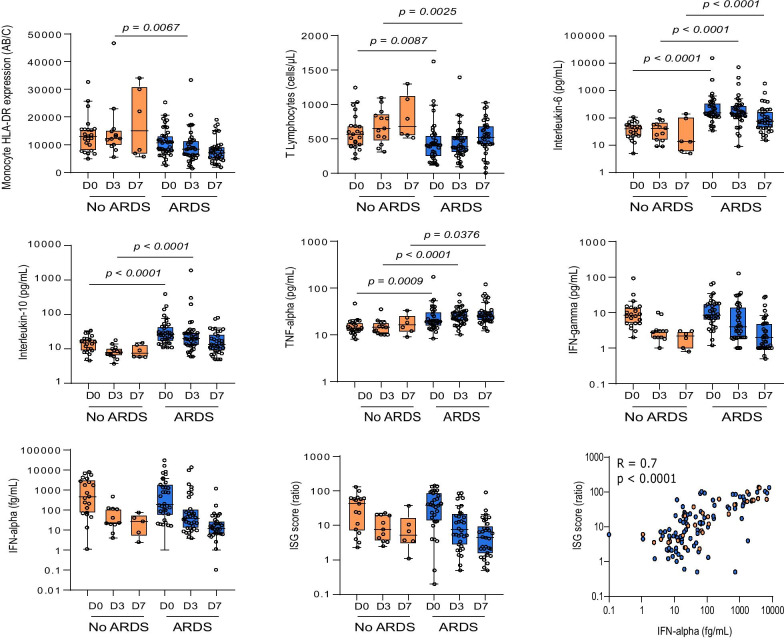
ARDS patients presented with persistently decreased lymphocyte count and mHLA-DR expression and increased cytokine levels. Type-I IFN response was initially induced with elevation of IFNα2 levels and ISG score followed by a rapid decrease over time. Survivors and non-survivors presented with apparent common immune responses over the first 3 weeks after ICU admission mixing gradual return to normal values of cellular markers and progressive decrease of cytokines levels including IFNα2. Only plasma TNF-α presented with a slow increase over time and higher values in non-survivors compared with survivors. This paralleled with an extremely high occurrence of secondary infections in COVID-19 patients with ARDS.
Occurrence of ARDS in response to SARS-CoV2 infection appears to be strongly associated with the intensity of immune alterations upon ICU admission of COVID-19 patients. In these critically ill patients, immune profile presents with similarities with the delayed step of immunosuppression described in bacterial sepsis.
自疫情爆发以来,仅有少数研究关注了急性呼吸窘迫综合征(ARDS)的 COVID-19 危重症患者的纵向免疫监测,而这些患者的住院时间可能长达数周。因此,免疫参数是否会导致或与这些危重症患者的预后延迟不良相关,这一问题仍未得到解答。
我们展示了 64 例 COVID-19 危重症患者的免疫炎症紊乱的动态描述,包括血浆 IFNα2 水平和 IFN 刺激基因(ISG)评分的测量。
ARDS 患者表现为持续的淋巴细胞计数和 mHLA-DR 表达降低,细胞因子水平升高。I 型 IFN 反应最初表现为 IFNα2 水平和 ISG 评分升高,随后随时间迅速下降。幸存者和非幸存者在 ICU 入院后前 3 周表现出明显的共同免疫反应,细胞标志物逐渐恢复正常,细胞因子水平(包括 IFNα2)逐渐下降。只有 TNF-α在血浆中随时间呈缓慢增加,且非幸存者的水平高于幸存者。这与 COVID-19 合并 ARDS 患者继发感染的极高发生率相平行。
SARS-CoV2 感染导致的 ARDS 似乎与 COVID-19 患者 ICU 入院时免疫改变的强度密切相关。在这些危重症患者中,免疫谱与细菌脓毒症中描述的免疫抑制延迟阶段具有相似性。