Département Immunologie-Hématologie Hôpitaux Universitaires Henri Mondor.
INSERM U955 Team 16, Créteil, France.
Am J Respir Crit Care Med. 2020 Dec 1;202(11):1509-1519. doi: 10.1164/rccm.202005-1885OC.
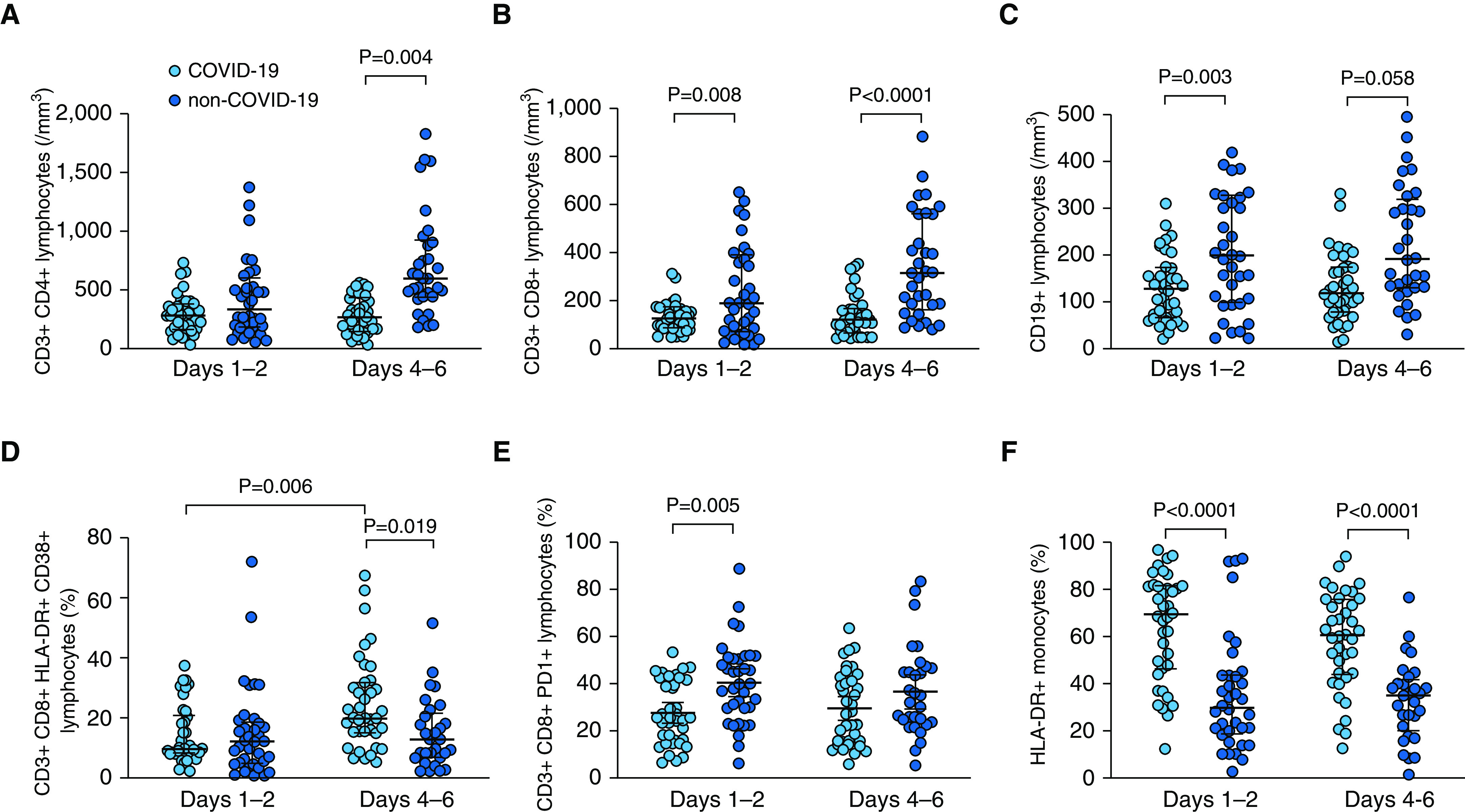
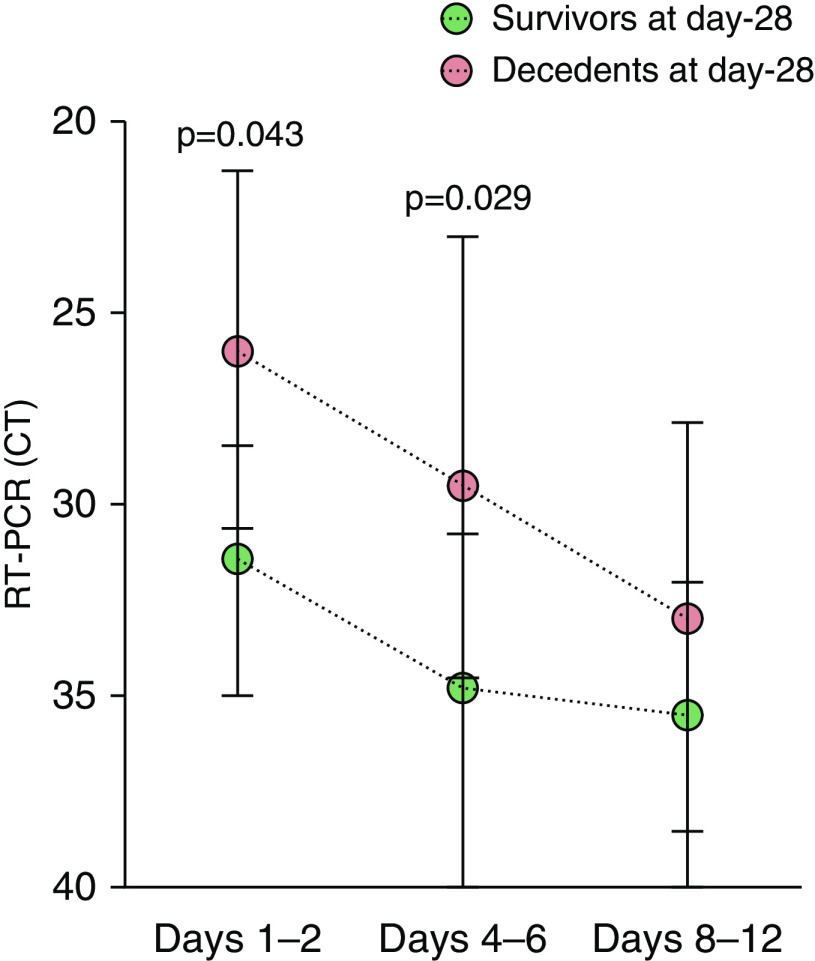
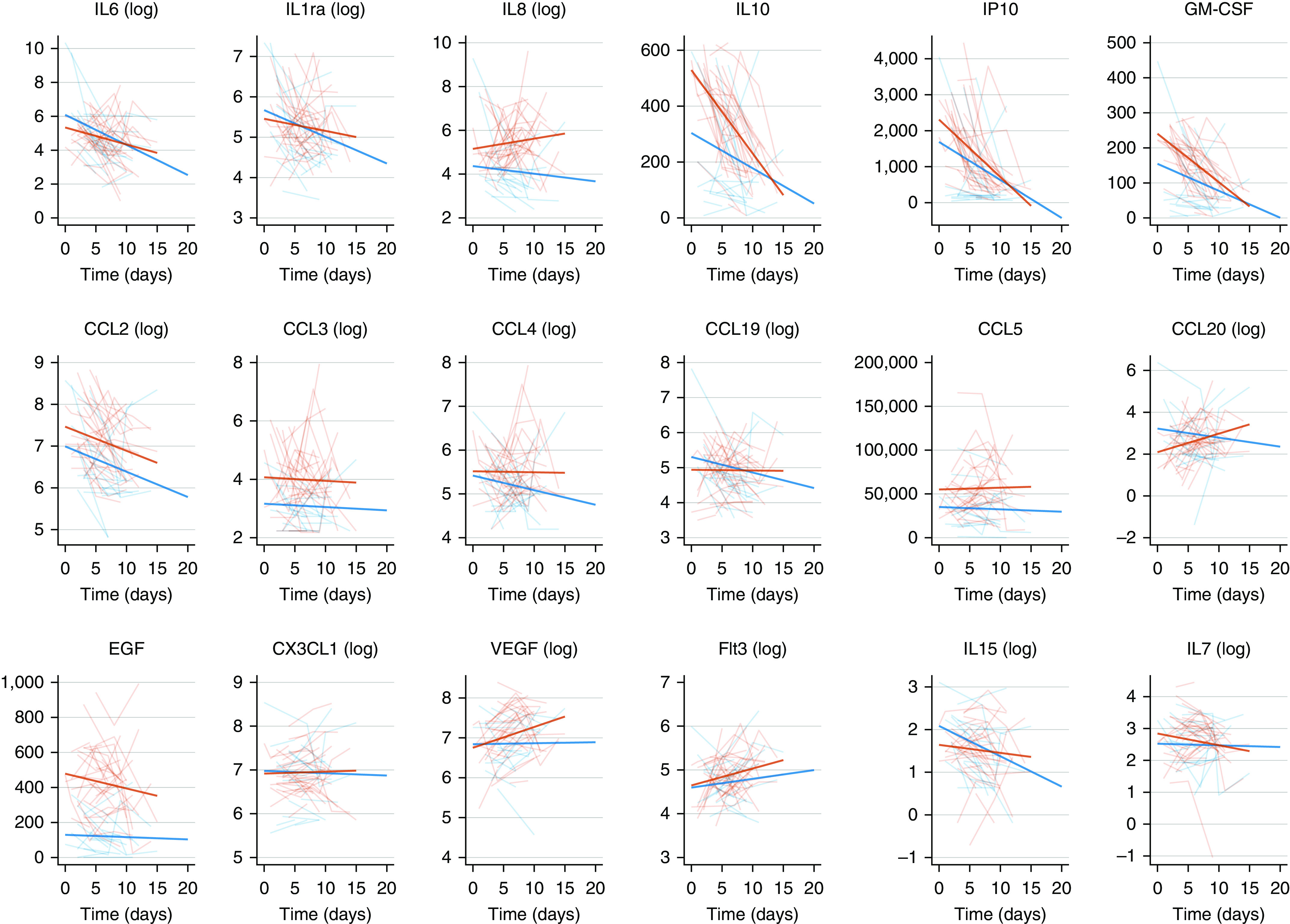
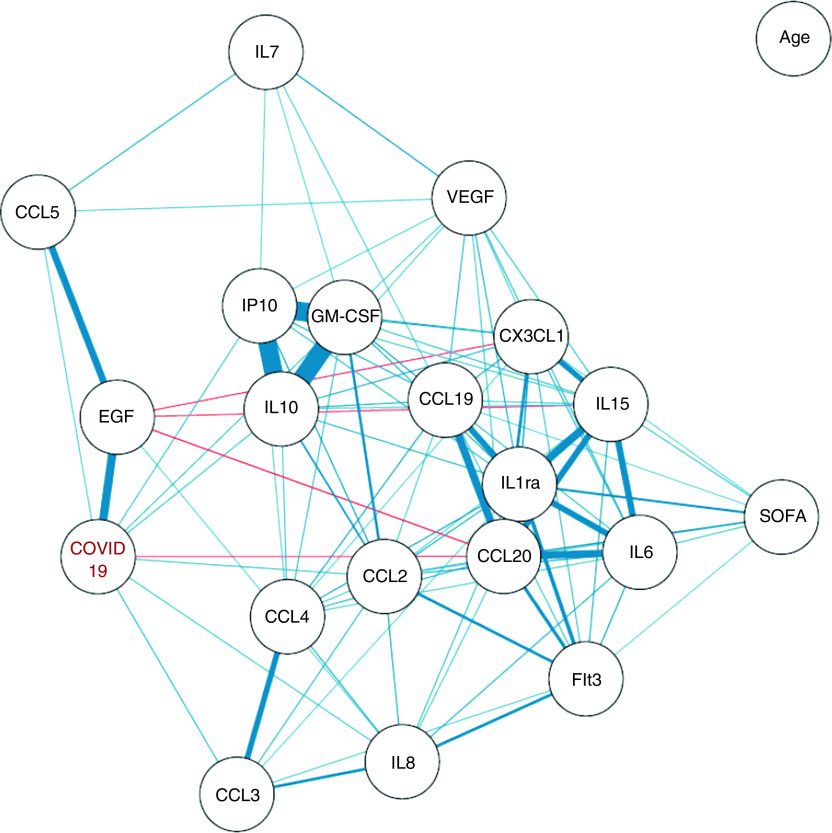
Uncontrolled inflammatory innate response and impaired adaptive immune response are associated with clinical severity in patients with coronavirus disease (COVID-19). To compare the immunopathology of COVID-19 acute respiratory distress syndrome (ARDS) with that of non-COVID-19 ARDS, and to identify biomarkers associated with mortality in patients with COVID-19 ARDS. Prospective observational monocenter study. Immunocompetent patients diagnosed with RT-PCR-confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and ARDS admitted between March 8 and March 30, 2020, were included and compared with patients with non-COVID-19 ARDS. The primary clinical endpoint of the study was mortality at Day 28. Flow cytometry analyses and serum cytokine measurements were performed at Days 1-2 and 4-6 of ICU admission. As compared with patients with non-COVID-19 ARDS ( = 36), those with COVID-19 ( = 38) were not significantly different regarding age, sex, and Sequential Organ Failure Assessment and Simplified Acute Physiology Score II scores but exhibited a higher Day-28 mortality (34% vs. 11%, = 0.030). Patients with COVID-19 showed profound and sustained T CD4 ( = 0.002), CD8 ( < 0.0001), and B ( < 0.0001) lymphopenia, higher HLA-DR expression on monocytes ( < 0.001) and higher serum concentrations of EGF (epithelial growth factor), GM-CSF, IL-10, CCL2/MCP-1, CCL3/MIP-1a, CXCL10/IP-10, CCL5/RANTES, and CCL20/MIP-3a. After adjusting on age and Sequential Organ Failure Assessment, serum CXCL10/IP-10 ( = 0.047) and GM-CSF ( = 0.050) were higher and nasopharyngeal RT-PCR cycle threshold values lower ( = 0.010) in patients with COVID-19 who were dead at Day 28. Profound global lymphopenia and a "chemokine signature" were observed in COVID-19 ARDS. Increased serum concentrations of CXCL10/IP-10 and GM-CSF, together with higher nasopharyngeal SARS-CoV-2 viral load, were associated with Day-28 mortality.
未控制的炎症固有反应和受损的适应性免疫反应与冠状病毒病(COVID-19)患者的临床严重程度相关。为了比较 COVID-19 急性呼吸窘迫综合征(ARDS)与非 COVID-19 ARDS 的免疫病理学,并确定与 COVID-19 ARDS 患者死亡率相关的生物标志物。前瞻性观察性单中心研究。纳入 2020 年 3 月 8 日至 3 月 30 日期间因经 RT-PCR 确诊的严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)感染和 ARDS 而住院的免疫功能正常的患者,并与非 COVID-19 ARDS 患者进行比较。研究的主要临床终点为第 28 天的死亡率。在 ICU 入院第 1-2 天和第 4-6 天进行流式细胞术分析和血清细胞因子测量。与非 COVID-19 ARDS 患者(n=36)相比,COVID-19 患者(n=38)在年龄、性别和序贯器官衰竭评估和简化急性生理学评分 II 方面无显著差异,但第 28 天死亡率较高(34% vs. 11%,=0.030)。COVID-19 患者表现出明显且持续的 CD4(=0.002)、CD8(<0.0001)和 B(<0.0001)淋巴细胞减少症,单核细胞上 HLA-DR 表达增加(<0.001),血清中 EGF(上皮生长因子)、GM-CSF、IL-10、CCL2/MCP-1、CCL3/MIP-1a、CXCL10/IP-10、CCL5/RANTES 和 CCL20/MIP-3a 浓度升高。在调整年龄和序贯器官衰竭评估后,COVID-19 患者死亡(=0.047)的血清 CXCL10/IP-10 和 GM-CSF(=0.050)更高,鼻咽 RT-PCR 循环阈值值更低(=0.010)。在 COVID-19 ARDS 中观察到广泛的全身淋巴细胞减少症和“趋化因子特征”。血清 CXCL10/IP-10 和 GM-CSF 浓度增加,以及鼻咽 SARS-CoV-2 病毒载量升高与第 28 天死亡率相关。