Unit of Clinical Epidemiology, IRCCS Istituto Ortopedico Galeazzi, Milano, Lombardia, Italy.
Unit of Clinical Epidemiology, IRCCS Istituto Ortopedico Galeazzi, Milano, Lombardia, Italy
Br J Sports Med. 2022 Jan;56(1):41-50. doi: 10.1136/bjsports-2020-103596. Epub 2021 Apr 13.
To assess the effectiveness of interventions for acute and subacute non-specific low back pain (NS-LBP) based on pain and disability outcomes.
A systematic review of the literature with network meta-analysis.
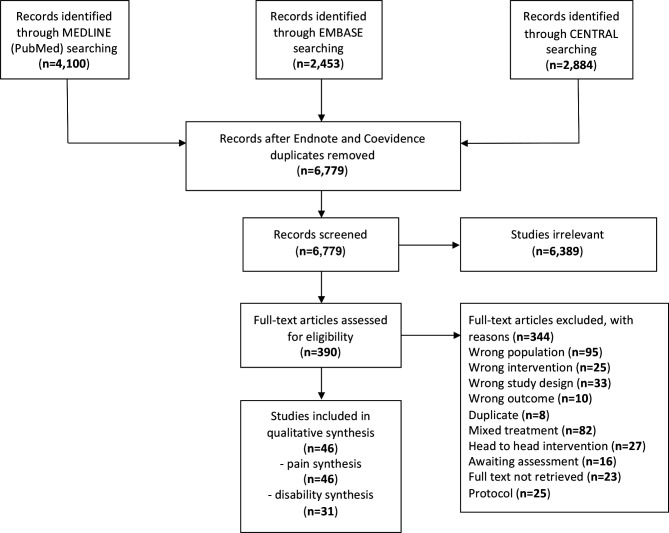
Medline, Embase and CENTRAL databases were searched from inception until 17 October 2020.
Randomised clinical trials (RCTs) involving adults with NS-LBP who experienced pain for less than 6 weeks (acute) or between 6 and 12 weeks (subacute).
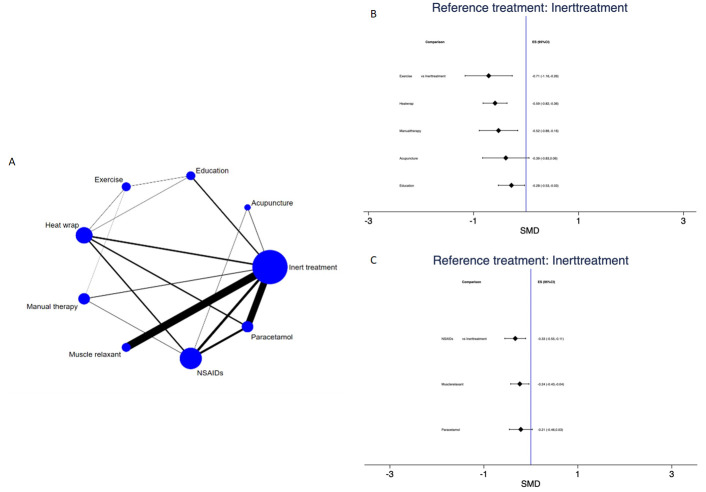
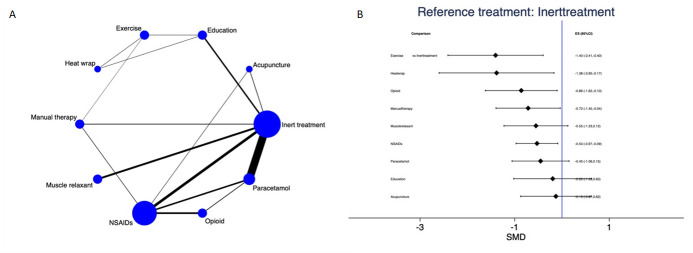
Forty-six RCTs (n=8765) were included; risk of bias was low in 9 trials (19.6%), unclear in 20 (43.5%), and high in 17 (36.9%). At immediate-term follow-up, for pain decrease, the most efficacious treatments against an inert therapy were: exercise (standardised mean difference (SMD) -1.40; 95% confidence interval (CI) -2.41 to -0.40), heat wrap (SMD -1.38; 95% CI -2.60 to -0.17), opioids (SMD -0.86; 95% CI -1.62 to -0.10), manual therapy (SMD -0.72; 95% CI -1.40 to -0.04) and non-steroidal anti-inflammatory drugs (NSAIDs) (SMD -0.53; 95% CI -0.97 to -0.09). Similar findings were confirmed for disability reduction in non-pharmacological and pharmacological networks, including muscle relaxants (SMD -0.24; 95% CI -0.43 to -0.04). Mild or moderate adverse events were reported in the opioids (65.7%), NSAIDs (54.3%) and steroids (46.9%) trial arms.
With uncertainty of evidence, NS-LBP should be managed with non-pharmacological treatments which seem to mitigate pain and disability at immediate-term. Among pharmacological interventions, NSAIDs and muscle relaxants appear to offer the best harm-benefit balance.
基于疼痛和残疾结局评估急性和亚急性非特异性下背痛(NS-LBP)干预措施的有效性。
系统文献综述与网络荟萃分析。
从创建到 2020 年 10 月 17 日,检索了 Medline、Embase 和 CENTRAL 数据库。
涉及疼痛时间少于 6 周(急性)或 6-12 周(亚急性)的 NS-LBP 成人的随机临床试验(RCT)。
纳入 46 项 RCT(n=8765);9 项试验(19.6%)的偏倚风险低,20 项试验(43.5%)的偏倚风险不明确,17 项试验(36.9%)的偏倚风险高。在即时随访时,对于疼痛减轻,与惰性治疗相比,最有效的治疗方法是:运动(标准化均数差(SMD)-1.40;95%置信区间(CI)-2.41 至-0.40)、热敷(SMD-1.38;95%CI-2.60 至-0.17)、阿片类药物(SMD-0.86;95%CI-1.62 至-0.10)、手法治疗(SMD-0.72;95%CI-1.40 至-0.04)和非甾体抗炎药(NSAIDs)(SMD-0.53;95%CI-0.97 至-0.09)。在非药物和药物网络中,包括肌肉松弛剂(SMD-0.24;95%CI-0.43 至-0.04),也证实了残疾减轻的类似发现。在阿片类药物(65.7%)、非甾体抗炎药(54.3%)和类固醇(46.9%)试验组中报告了轻度或中度不良反应。
由于证据存在不确定性,NS-LBP 应采用非药物治疗,这似乎可以减轻即时疼痛和残疾。在药物干预中,NSAIDs 和肌肉松弛剂似乎提供了最佳的利弊平衡。