Schuler Thilo, Back Michael, Hruby George, Carroll Susan, Jayamanne Dasantha, Kneebone Andrew, Stevens Mark, Lamoury Gillian, Morgia Marita, Wong Shelley, Grimberg Kylie, Roderick Stephanie, Booth Jeremy, Eade Thomas
Northern Sydney Cancer Centre, Royal North Shore Hospital, Sydney, Australia.
Australian Institute of Health Innovation, Macquarie University, Sydney, Australia.
Adv Radiat Oncol. 2020 Dec 3;6(2):100632. doi: 10.1016/j.adro.2020.100632. eCollection 2021 Mar-Apr.
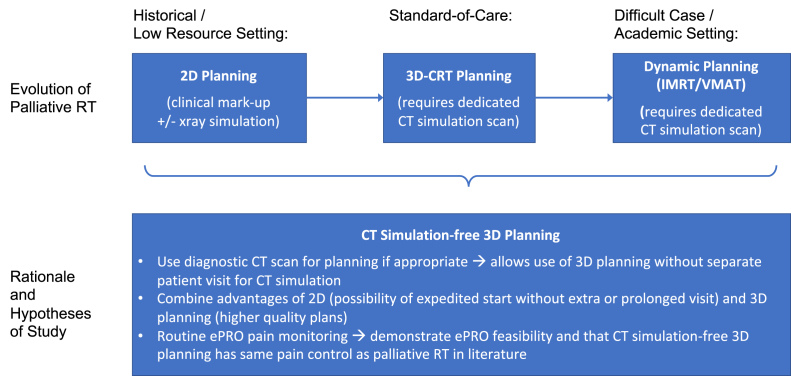
Our purpose was to report outcomes of a novel palliative radiation therapy protocol that omits computed tomography simulation and prospectively collects electronic patient-reported outcomes (ePROs).
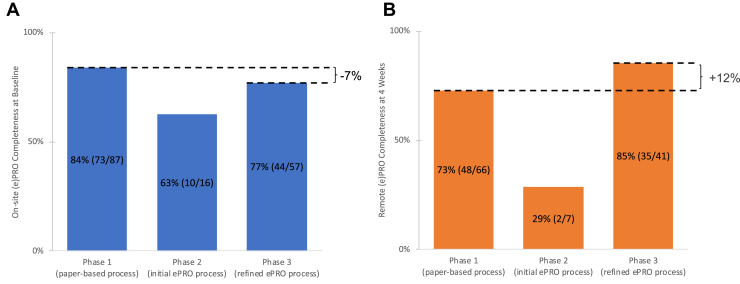
Patients receiving extracranial, nonstereotactic, linear accelerator-based palliative radiation therapy who met inclusion criteria (no mask-based immobilization and a diagnostic computed tomography within 4 weeks) were eligible. Global pain was scored with the 11-point numerical pain rating scale (NPRS). Patients were coded as having osseous or soft tissue metastases and no/mild versus severe baseline pain (NPRS ≥ 5). Pain response at 4 weeks was measured according to the international consensus (no analgesia adjustment). Transition to ePRO questionnaires was completed in 3 phases. Initially, pain assessments were collected on paper for 11 months, then pilot ePROs for 1 month and then, after adjustments, revised ePROs from 1 year onwards. ePRO feasibility criteria were established with reference to the paper-based process and published evidence.
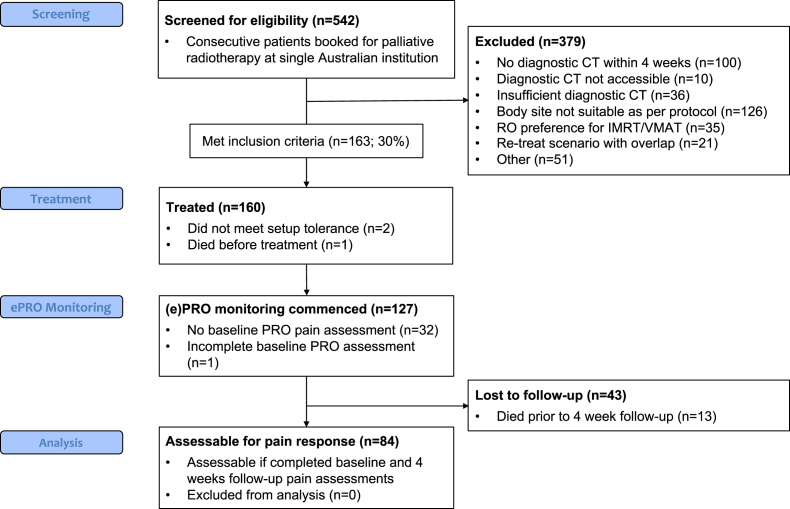
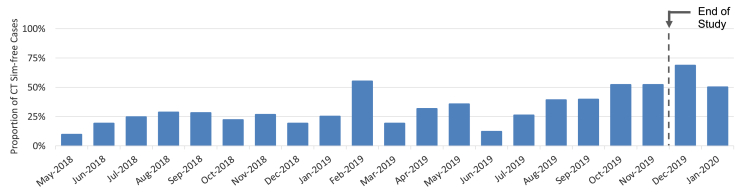
Between May 2018 and November 2019, 542 consecutive patients were screened, of whom 163 were eligible (30%), and 160 patients were successfully treated. The proportion of patients eligible for the study improved from approximately 20% to 50% by study end. Routine care pain monitoring via ePROs was feasible. One hundred twenty-seven patients had a baseline NPRS recording. Ninety-five patients had osseous (61% severe pain) and 32 had soft tissue (25% severe pain) metastases. Eighty-four patients (66%) were assessable for pain response at 4 weeks. In the 41 patients with severe osseous pain, overall and complete pain response was 78% and 22%, respectively.
By study completion, 50% of patients receiving palliative extracranial radiation therapy avoided simulation, streamlining the treatment process and maximizing patient convenience. Pain response for patients with severe pain from osseous lesions was equivalent to published evidence.
我们的目的是报告一种新型姑息性放射治疗方案的结果,该方案省略了计算机断层扫描模拟,并前瞻性地收集患者电子报告结局(ePROs)。
符合纳入标准(无需面罩固定且在4周内进行过诊断性计算机断层扫描)的接受颅外、非立体定向、基于直线加速器的姑息性放射治疗的患者符合条件。采用11点数字疼痛评分量表(NPRS)对总体疼痛进行评分。患者被编码为有骨转移或软组织转移,以及无/轻度与重度基线疼痛(NPRS≥5)。4周时的疼痛反应根据国际共识进行测量(无需调整镇痛药物)。向ePRO问卷的过渡分三个阶段完成。最初,纸质疼痛评估收集了11个月,然后进行了1个月的ePRO试点,之后经过调整,从第1年起采用修订后的ePRO。参照纸质流程和已发表的证据确定了ePRO可行性标准。
2018年5月至2019年11月期间,连续筛查了542例患者,其中163例符合条件(30%),160例患者成功接受治疗。到研究结束时,符合研究条件的患者比例从约20%提高到了50%。通过ePRO进行常规护理疼痛监测是可行的。127例患者有基线NPRS记录。95例患者有骨转移(61%为重度疼痛),32例有软组织转移(25%为重度疼痛)。84例患者(66%)在4周时可评估疼痛反应。在41例重度骨痛患者中,总体疼痛缓解率和完全疼痛缓解率分别为78%和22%。
到研究完成时,50%接受姑息性颅外放射治疗的患者避免了模拟,简化了治疗过程并最大限度地方便了患者。骨病变引起的重度疼痛患者的疼痛缓解情况与已发表的证据相当。