Department of Physical Therapy, Federal University of Minas Gerais (UFMG), Av. Antônio Carlos 6627, EEFFTO, Pampulha, Belo Horizonte, Minas Gerais, Brazil.
Faculty of Medicine, Federal University of Minas Gerais (UFMG), Belo Horizonte, Minas Gerais, Brazil.
BMC Geriatr. 2021 Apr 14;21(1):246. doi: 10.1186/s12877-021-02193-y.
Frailty is a predictor of negative health outcomes in older adults. The physical frailty phenotype is an often used form for its operationalization. Some authors have pointed out limitations regarding the unidimensionality of the physical phenotype, introducing other dimensions in the approach to frailty. This study aimed to create a multidimensional model to evaluate frailty in older Brazilian adults and to compare the dimensions of the model created among the categories of the physical frailty phenotype.
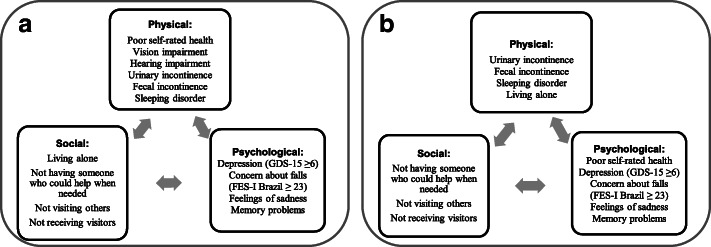
A cross-sectional study was conducted using data from 3569 participants (73.7 ± 6.6 years) from a multicenter and multidisciplinary survey (FIBRA-BR). A three-dimensional model was developed: physical dimension (poor self-rated health, vision impairment, hearing impairment, urinary incontinence, fecal incontinence, and sleeping disorder), social dimension (living alone, not having someone who could help when needed, not visiting others, and not receiving visitors), and psychological dimension (depressive symptoms, concern about falls, feelings of sadness, and memory problems). The five criteria of the phenotype created by Fried and colleagues were used to evaluate the physical frailty phenotype. The proposed multidimensional frailty model was analyzed using factorial analysis. Pearson's chi-square test was used to analyze the associations between each variable of the multidimensional frailty model and the physical phenotype categories. Analysis of variance compared the multidimensional dimensions scores among the three categories of the physical frailty phenotype.
The factorial analysis confirmed a model with three factors, composed of 12 variables, which explained 38.6% of the variability of the model data. The self-rated health variable was transferred to the psychological dimension and living alone variable to the physical dimension. The vision impairment and hearing impairment variables were dropped from the physical dimension. The variables significantly associated with the physical phenotype were self-rated health, urinary incontinence, visiting others, receiving visitors, depressive symptoms, concern about falls, feelings of sadness, and memory problems. A statistically significant difference in mean scores for physical, social, and psychological dimensions among three physical phenotype categories was observed (p < 0.001).
These results confirm the applicability of our frailty model and suggest the need for a multidimensional approach to providing appropriate and comprehensive care for older adults.
衰弱是老年人健康不良后果的预测因素。身体衰弱表型是其操作的常用形式。一些作者指出了身体表型的非多维性的局限性,在衰弱的方法中引入了其他维度。本研究旨在创建一个多维模型来评估巴西老年人的衰弱,并比较在身体衰弱表型类别中创建的模型的维度。
使用来自多中心和多学科调查(FIBRA-BR)的 3569 名参与者(73.7±6.6 岁)的数据进行了横断面研究。开发了一个三维模型:身体维度(自我报告的健康状况不佳、视力障碍、听力障碍、尿失禁、大便失禁和睡眠障碍)、社会维度(独居、需要帮助时无人可求助、不拜访他人、不接待访客)和心理维度(抑郁症状、对跌倒的担忧、悲伤感和记忆力问题)。使用 Fried 及其同事创建的表型的五个标准评估身体衰弱表型。使用因子分析对所提出的多维衰弱模型进行分析。Pearson 卡方检验用于分析多维衰弱模型的每个变量与身体表型类别的关联。方差分析比较了身体衰弱表型的三个类别之间多维维度分数的差异。
因子分析证实了一个具有三个因子的模型,由 12 个变量组成,解释了模型数据变异性的 38.6%。自我报告的健康状况变量转移到心理维度,独居变量转移到身体维度。视觉障碍和听力障碍变量从身体维度中删除。与身体表型显著相关的变量是自我报告的健康状况、尿失禁、拜访他人、接待访客、抑郁症状、对跌倒的担忧、悲伤感和记忆力问题。在三个身体表型类别中,身体、社会和心理维度的平均得分存在统计学显著差异(p<0.001)。
这些结果证实了我们的衰弱模型的适用性,并表明需要采用多维方法为老年人提供适当和全面的护理。