Pritzker School of Medicine, University of Chicago, Chicago, Illinois.
Department of Medicine, UT San Antonio, San Antonio, Texas.
Am J Transplant. 2021 Nov;21(11):3684-3693. doi: 10.1111/ajt.16614. Epub 2021 May 5.
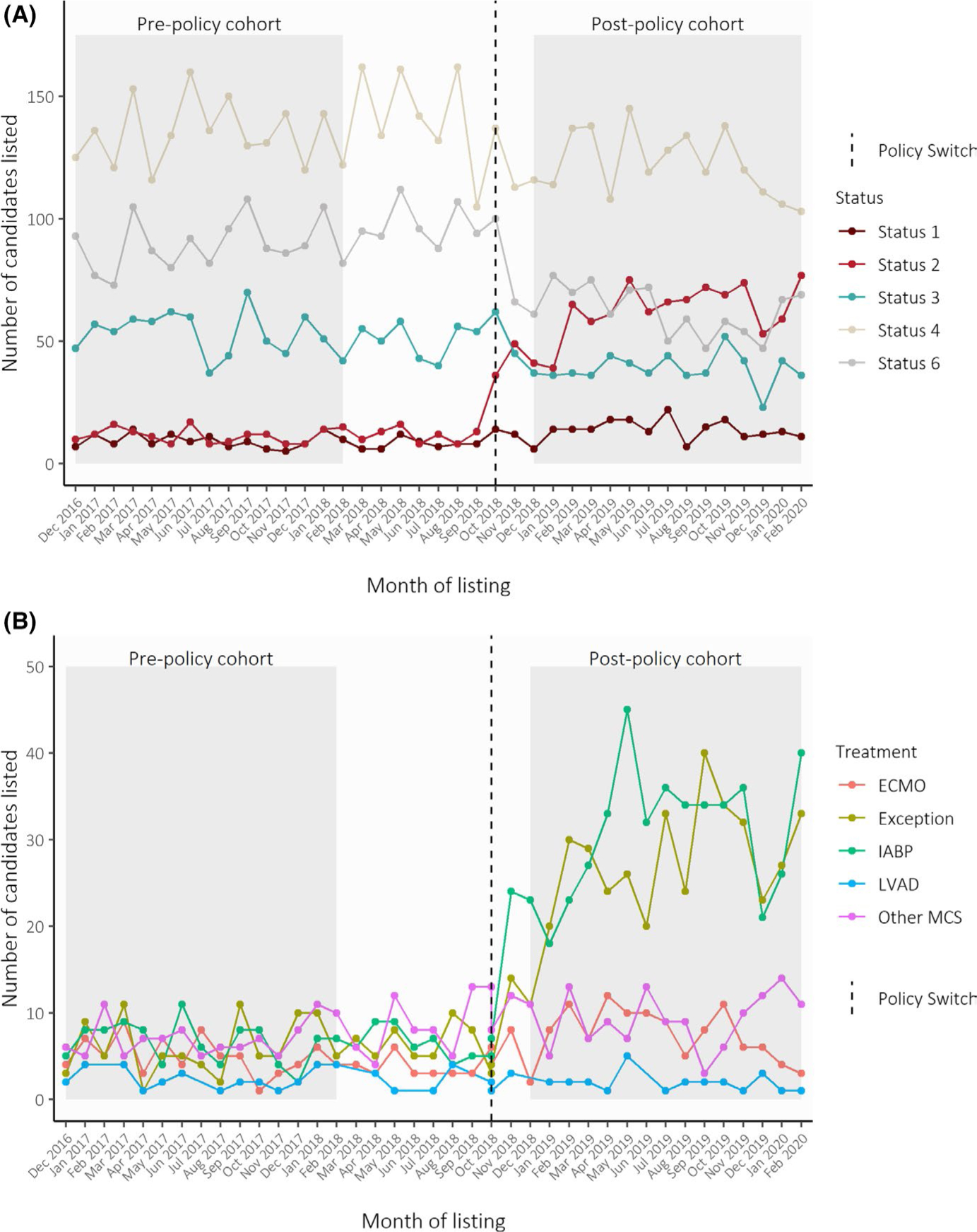
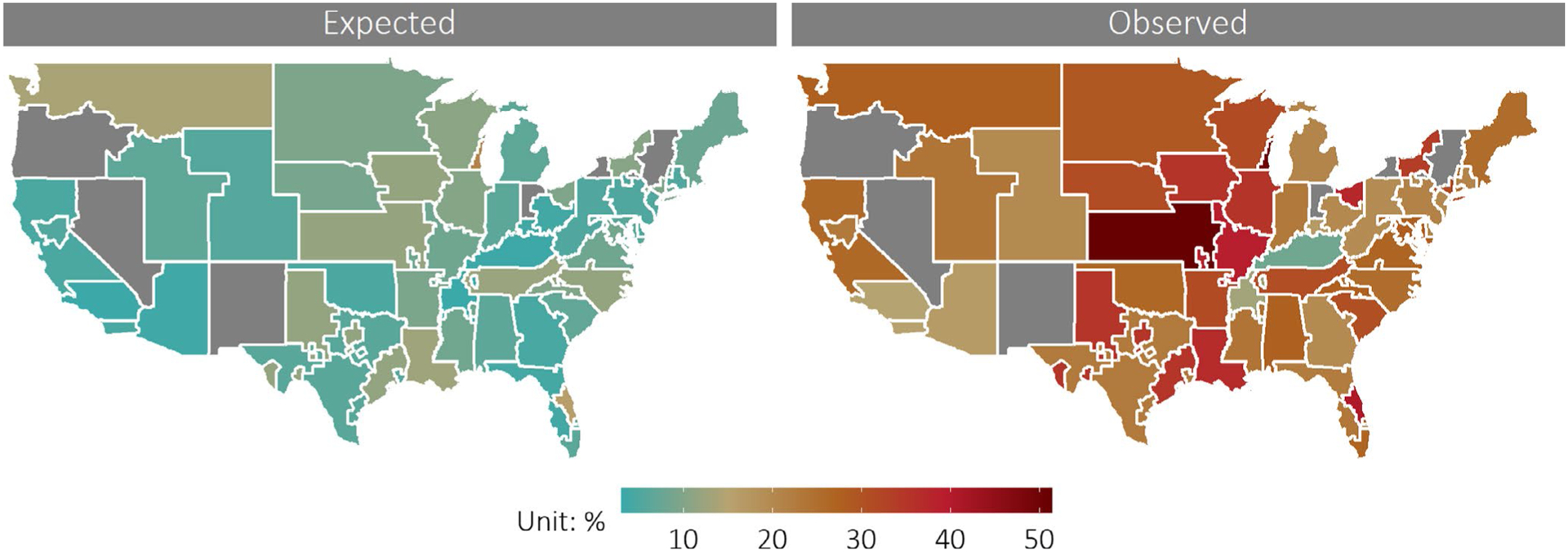
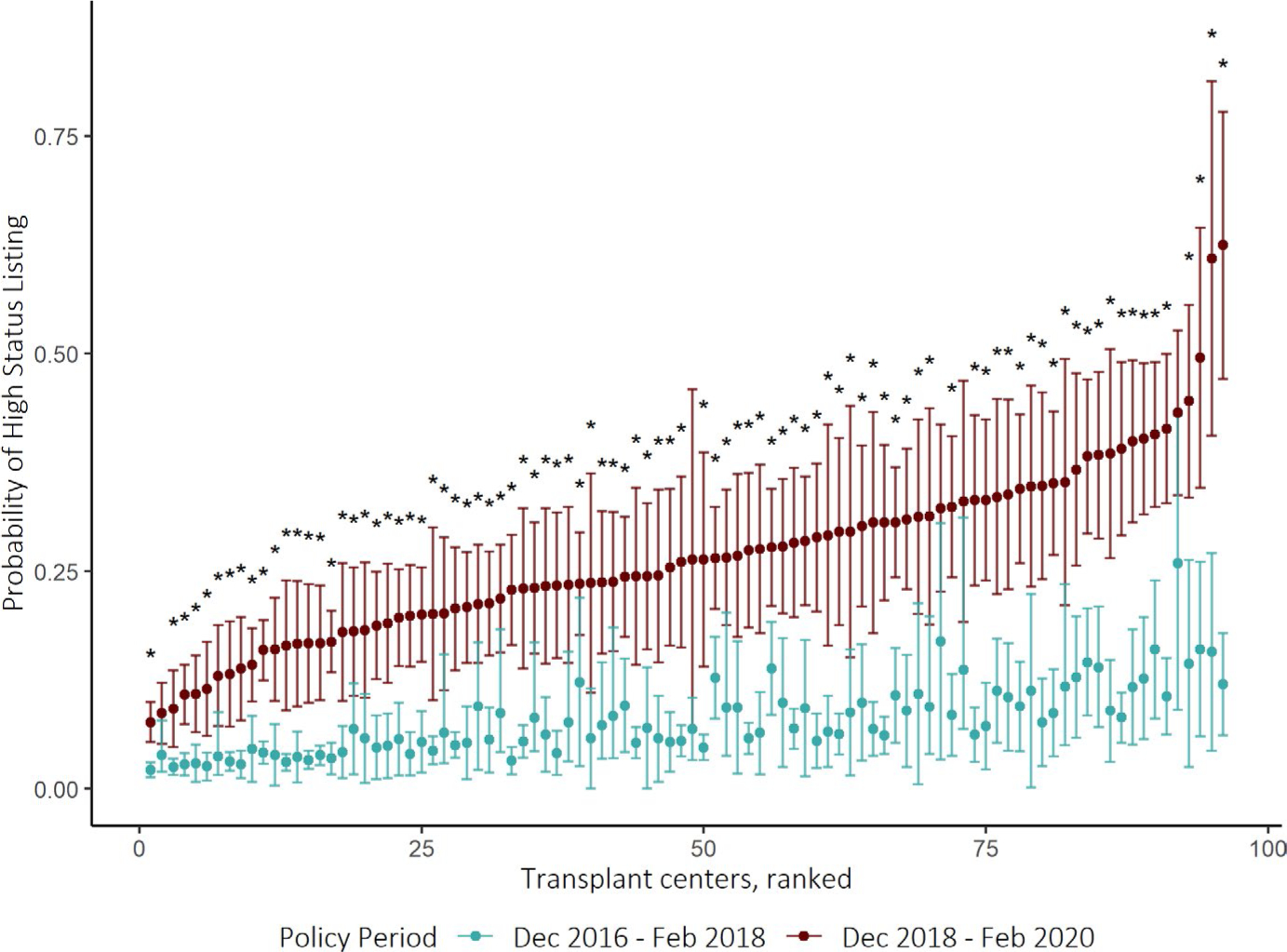
Under the new US heart allocation policy, transplant centers listed significantly more candidates at high priority statuses (Status 1 and 2) with mechanical circulatory support devices than expected. We determined whether the practice change was widespread or concentrated among certain transplant centers. Using data from the Scientific Registry of Transplant Recipients, we used mixed-effect logistic regression to compare the observed listings of adult, heart-alone transplant candidates post-policy (December 2018 to February 2020) to seasonally matched pre-policy cohort (December 2016 to February 2018). US transplant centers (N = 96) listed similar number of candidates in each policy period (4472 vs. 4498) but listed significantly more at high priority status (25.5% vs. 7.0%, p < .001) than expected. Adjusted for candidate characteristics, 91 of 96 (94.8%) centers listed significantly more candidates at high-priority status than expected, with the unexpected increase varying from 4.8% to 50.4% (interquartile range [IQR]: 14.0%-23.3%). Centers in OPOs with highest Status 1A transplant rate pre-policy were significantly more likely to utilize high-priority status under the new policy (OR: 9.73, p = .01). The new heart allocation policy was associated with widespread and significantly variable changes in transplant center practice that may undermine the effectiveness of the new system.
根据美国新的心脏分配政策,移植中心列出的具有机械循环支持装置的高优先级状态(1 级和 2 级)的候选人数明显高于预期。我们确定这种做法的改变是广泛的还是集中在某些移植中心。我们使用移植受者科学登记处的数据,使用混合效应逻辑回归来比较政策后(2018 年 12 月至 2020 年 2 月)成人、心脏单独移植候选者的观察列表与政策前季节性匹配队列(2016 年 12 月至 2018 年 2 月)。美国移植中心(N=96)在每个政策期列出的候选人数相似(4472 与 4498),但在高优先级状态下列出的人数明显更多(25.5%与 7.0%,p<.001),超出预期。在调整候选者特征后,96 个中心中的 91 个(94.8%)列出的高优先级状态候选者明显多于预期,意外增加幅度从 4.8%到 50.4%(四分位距 [IQR]:14.0%-23.3%)。政策前具有最高 1A 级移植率的器官获取组织中,在新政策下更有可能利用高优先级状态(OR:9.73,p=.01)。新的心脏分配政策与移植中心实践的广泛且显著变化相关,这可能会破坏新系统的有效性。